

Helo Hospital is part of a multistate hospital system that has been adding 5 to 10 hospitals
Question:
Helo Hospital is part of a multistate hospital system that has been adding 5 to 10 hospitals per year for the past decade. Originally, three local hospitals made up the company, and the largest hospital’s CEO supervised the heads of the other two facilities. When the system grew into 15 hospitals, the organization created a corporate office; when it grew into 30 hospitals, a multidivisional structure based on geography (east and west divisions) was adopted. Currently, disagreements have arisen regarding who should have control of specific services. In particular, the system is debating whether marketing, managed care contracting, strategic planning, business development, purchasing, biomedical maintenance, and recruiting should be centralized or decentralized. The executives from the hospitals and corporate office have scheduled a meeting to decide how these services should be allocated across the system. They have asked you to prepare a report on the advantages and disadvantages of placing these functions in a centralized corporate office, in the divisions, or at the hospital level. What are the problems and possible benefits of each arrangement?
Elizabeth was the chief nursing officer (CNO) of a large health system. Because of the complicated nature of its business in the past, she had led the restructuring of the patient care services across the system. Physicians and staff had expressed concerns that 10 of their hospitals often used nonevidence-based practices and were experiencing broad clinical variation. Her restructuring team was asked to create a structure that would facilitate improvements in clinical value, lower costs, decrease complication rates, and cut readmissions across all service lines. Stakeholders in the system perceived the result, which involved nine service lines, to be a great advance, with greater centralization and improved coordinative structures achieved through a modified service line management with clinical co-management.
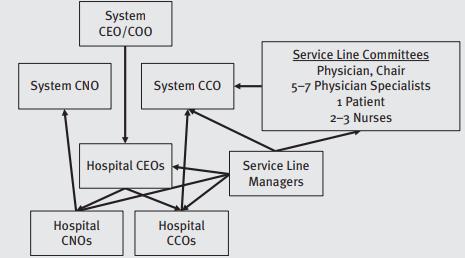
According to the design, a chief clinical officer (CCO) responsible for the full system oversaw teams responsible for each service line. Each service line contained several multidisciplinary program committees chaired by doctors and organized by medical condition systemwide. For instance, the cancer service line included subcommittees for breast, colon, and lung cancer clinical care. IT supported the subcommittees and informed them of clinical variation. Subcommittees also included at least one patient and three nurses. Additional support for subcommittees came from data analysts and performance improvement and pharmacy staff. Scorecards were made to show performance data on quality, finances, and patient experience. Those clinicians or service lines in specific hospitals not meeting expectations were referred to their respective administrative and clinical manager.
Nursing services were also grouped into a service line structure, but each hospital also had a CNO who reported to Elizabeth and the hospital CEO. A simplistic view of the structure looks like the following:
Questions
1. According to what you have learned in this chapter, what are some of the structural challenges of implementing such a structure?
2. Why would two of the service lines appear to have success while others fail?
3. What suggestions might you have to improve the success of this organization?
Step by Step Answer:
Strategic Management Helo Hospital is facing a dilemma on whether to adopt a centralized or decentralized structure for major functions in the hospital such as strategic planning marketing recruiting ...View the full answer


Strategic Healthcare Management Planning And Execution
ISBN: 9781640553651
3rd Edition
Authors: Stephen L. Walston PhD
