Question: After reading: Risk-Shifting in Health Care and its Implications and Its Not Just Risk - Why the Shift to Value-Based Payment is also About Provider
After reading:
- Risk-Shifting in Health Care and its Implications and
- Its Not Just Risk - Why the Shift to Value-Based Payment is also About Provider Flexibility
Answer the following question.
How would you reduce financial risk for providers (you must cite material from both articles)?
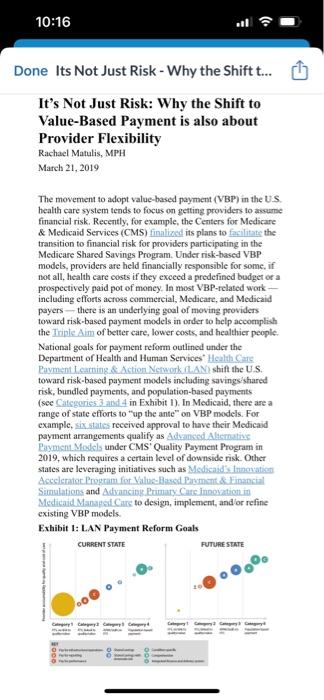
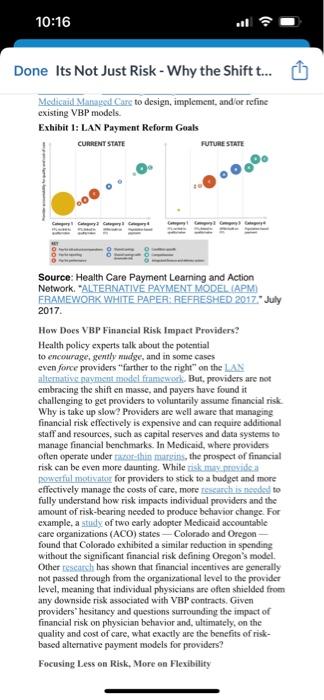
Risk-Shifting in Health Care and its Implications AUGUST 24, 2011 We believe that the most striking changes will eccur in the locus of risk for poor health. For the past 40 years, much of that has been held by the insurers, employer and the government acting as insurer. Every sign today is that risk will begin to move to consumers, and to providers, the latter in the form of what is today called an accountable care organization. Health reform appears to be speeding the migration of risk. Accountable Care Organizations: A Shift of Risk to Providers What we see with the PPACA's endorsement of, and focus on, accountable care organizations is an effort to move half or more of the risk for the quality and costs of health eare to peoviders. This was attempted before, in the Clinton Administration's proposed Health Security Act, but in the late 1990's global capitation for providers largely failed. Of course, the financial situation for the country was radically different at the time; hage deficits were not impelling reform. The call for accountable care organizations is based on the widely accepted notion that bealth care inflation is based on foefor-service payment methods. Under fec for service, providers get paid more for doing more, and so they do more. But "more" often involves unnecessary or wasteful care that brings little health value. The hope for accountable care organizations is that by making providers responsible for the health of a population, and paying them on a fixed budget, they will adjust their choises about therapy, providing only that which is necessary. This prospect brings the accountable care organization concept bipartisan support, although some continue to harbor the suspicions from our last effort at "mantiged care" in the 1990 .s. The Potential Shift of Risk to the Paticent The other potential risk bearer is the individual patient, who would be encouraged to have "more skin in the game" by having higher deductibles, copayments, and co-insurance, and thereby make more coss-effective decisions about health care. The same effect oecurs when Medieare becomes a defined contribution, under the Ryan plan, rather than a defined benefit. Underlying these programs is the assumption that "thick" insurance coverage for the individual has created moral hazard: insulated from costs of the care, the individual chooses to have any prosedure or test the doctor recommends, and there is little shopping for low cost services. Creating higher deductibles puts the patient at risk for costs, and forces him or her to spend time locating lower cost approaches to treatment. The wide variation in costs for procedures even within discrete metropolitan areas provides a real basis for savings, and the threat that patients might "shop" in this manner forces providers The other potential risk bearer is the indrvidual patient, who would be cneouraged to have "mote skin in the game" by having higher deductibles, cogayments, and co-insurance, and thereby make more cosh-effective decissons about health care. The same effect occurs when Medicare becomes a defined contribution, under the Ryan plan, rather than a defined benefit. Underlying these programs is the assumption that "thick" insurance coverage for the individual has created moral harard: insulated from costs of the care, the individual chooses to have amy procedure of test the doctor recommends, and there is listle shopping for low cost services. Creating higher deductibles puts the patient at risk for costs, and forces him or her to spend time locating lover cost approaches to treatment. The wide variation in costs for procedures even within discrete metropolitan areas provides a real basis for savings, and the threat that patients might "shop" in this manner forces providers to recxartine and try to reduce their cost structures. Of course, most such plans limit the out-of-pocket expense at some level, which is usually quite a bit lower than spending for the sickest 70 percent of Americans in a given year. So consumer activity is limited by morbidity, but will impact a good deal of ambulatory, discretionary health care. Nonetheless, the prospect of shift of risk, helps explain much of what we see business, insurers (including the goverarnent) and providers doing today to address reform. And- despite freyuent assertions that the concept of accountable care onganizaticns remains to be defined, and complaints about first efforts to do se - the mosement towand accountable care organizations appeass to us to be even more likely than when the debate over bealh care teform begati. In the end, this risk shift should change the role of traditional insurers. We can expect them to move more toward providers; of more toward being "consumet information" cotspanies. Recent information suggests both moses atse mitorway . In suimmary, substantial change is incvitable in our health care system, given that we just carnsot afford our current system of care. It will affect patients, providers and insurers, all in different ways, and a great deal will tarn on exactly where the risk for illness resides. Providers As reform unfolds, providers are concemed about threats to theif ability to provide good care to their paticats in their traditional fashion - and that of course translates into concern aboat reimbursement. Implicitly, they understand the segment dynamics, and most have concluded that the federal programes will have negative margins goong forward. So they must continue to try to capture the private-pay scements - currently. the large exiployer self insured market and the fully insured market. But what happens to those sourees of cross-subsidies as the Providers As reform unfolds, providers are concerned about threats to their ability to provide good care to their patients in their traditional fashion - and that of course translates into concem about reimbursement. Implicitly, they understand the segment dynamics, and nost have concluded that the foderal programs will have negative margins going forward. So they must continue to try to capture the privase-pay scgments - currently, the large employer self insured market and the fully insured market. But what happens to those sources of cross-subsidies as the exchanges take shape and insurers face pressure to moderate premiums (similar to Massachusets), and if the large employers begin to "dump"? What happens if employers accelerate their shifting of risk to patients, thereby encouraging them to move market share to lower cost providers? What happens when individual mandates make prices charged by providers a favorite focus for political leaders? There is no cross-subsidy in this environment, and provider reimbursement simply drops. A strategy with a limeted lifespan? Faced with rising costs of their own. providers are unlikely to accept decreased resimbursement passively. Most will bargais hard with instaress who represent fully insured and self-insured employers, to make up for the moderation of government programs, In some geographic areas, haspitals have consolidated into syetcmis. often with affiliated medical groups, in part at least to gain negotiating effectivencss. However, this negotiation strategy may have reached its limits as further gains will only make employers, who have to pay for the higher rates eventually, less interested in staying in the health benefit game. Employers who linger are increasingly served by plans that use limits on benefits to drive employees to use lower-cost institutions. Thus, high-oost institutions are likely to see their demand efface in such a situation. The mavement taward accountable care organisations, As providers realize that the combisation of fiscal austerity and the impulses of the PPACA are changing the familar rules of private insurer negotiating and cross-subsidy of govemmens programs, their interest in accountable bealth care organizations (ACO's) grows. That dynamic is surely manifest in Massachusetts, where the rate of movement in this direction in commercial contracts has bect surprisingly fast. Now, that movement may be accelerated even more by the federal government's efforts. The. PeaC A cnderiod the ACD enncored and required CMS to develop a national program for ACO's by January, 2012. The initial regulations for accountable care organization were released in carly April, and many provider organitations hame underyhelmod. to say the least. The majority complained that the degree of regulation seemed burdensome and the return on imvestment small even in the most antmiction comarios. The movement roward accoumrable care orgarizarions. As providers realize that the combination of fiscal austerity and the impulses of the PBACA are changing the familiar nules of private insurer negotiating and cross-subsidy of governmeti programs, theit interest in accountable health care organizations (ACO's) grows. That dynamic is surely manifest in Massachusetts, where the rate of movement in this direction in commercial contracts has been surprisingly fast. Now, that movement may be accelerated even more by the federal governmen's efforts. The PRACA endarsed the ACO concegs and required CMS to develop a national program for ACO's by January, 2012. The initial regulations for accountable care organization were released in early April, and many provider ofganizations wers underwhelmed. to say the lenst. The majority cocoplained that the degree of regulation seemed burdensome and the return on investment small even in the most optimistic scenarios. In response, the Center for Medicare and Medicaid Services has developed a much more flevible model. Galled the Pioncer ACO frogenm, demonstrating the government's recognition that the ACO model is critical to controlling costs under the PPAC A. What lies immediately abead for ofganizations who subenit applications in July will be intense negotiating and planning betiore final goino-go decisions are made by December 31, 2011. ACO s are the fundamental vehicle in the PPACA to move away from fec-for-service medicine and its incentives for over-ase of care. The ACO curbs on cost would be hased, on the one hand, on bonuses for hitting quality and cost bencharmarks; and on the other as provider global budget rikk, i.e, capitation. The disadvantage of the former is that there are still precious few uncontroversial quality measures for hospitals, and oven ferwer. for ind ividual poysicians. and their ability to reduce costs is unproven. The advantage of the latter is that it is already an operational model in some parts of the country; the disaduantage is that it requires a large target patient popelation (to have an actuarially stable group) and integrated providers with the business acumen and financial reserves to bear financial risk. The good news for ACO advocates is that in many metropolitaz areas, the integrated delivery systems have already assembled the pieces to take capitation - they have size and physicianthospital eombinations, Organizithg these componcats into an ACO that can bear financial risk is still no small task, but it is at least imagirsable. Indecd, for such organizations, an argument for becoming a Medicare ACO is that such a commitment enhances their chances for success in commercial global budget contracts. The mote soptisticated potcitial ACOmight also realine that they could grow margin by climinating unnecessary care under capitation, and perhaps earn a hagher percentage of the health care dollar. Insurers, faced with more stringent regulations en MLR's, might be willing to tum some of their cost cutting The movement roward accoumrable care orgarizarions. As providers realize that the combination of fiscal austerity and the impulses of the PBACA are changing the familiar nules of private insurer negotiating and cross-subsidy of governmeti programs, theit interest in accountable health care organizations (ACO's) grows. That dynamic is surely manifest in Massachusetts, where the rate of movement in this direction in commercial contracts has been surprisingly fast. Now, that movement may be accelerated even more by the federal governmen's efforts. The PRACA endarsed the ACO concegs and required CMS to develop a national program for ACO's by January, 2012. The initial regulations for accountable care organization were released in early April, and many provider ofganizations wers underwhelmed. to say the lenst. The majority cocoplained that the degree of regulation seemed burdensome and the return on investment small even in the most optimistic scenarios. In response, the Center for Medicare and Medicaid Services has developed a much more flevible model. Galled the Pioncer ACO frogenm, demonstrating the government's recognition that the ACO model is critical to controlling costs under the PPAC A. What lies immediately abead for ofganizations who subenit applications in July will be intense negotiating and planning betiore final goino-go decisions are made by December 31, 2011. ACO s are the fundamental vehicle in the PPACA to move away from fec-for-service medicine and its incentives for over-ase of care. The ACO curbs on cost would be hased, on the one hand, on bonuses for hitting quality and cost bencharmarks; and on the other as provider global budget rikk, i.e, capitation. The disadvantage of the former is that there are still precious few uncontroversial quality measures for hospitals, and oven ferwer. for ind ividual poysicians. and their ability to reduce costs is unproven. The advantage of the latter is that it is already an operational model in some parts of the country; the disaduantage is that it requires a large target patient popelation (to have an actuarially stable group) and integrated providers with the business acumen and financial reserves to bear financial risk. The good news for ACO advocates is that in many metropolitaz areas, the integrated delivery systems have already assembled the pieces to take capitation - they have size and physicianthospital eombinations, Organizithg these componcats into an ACO that can bear financial risk is still no small task, but it is at least imagirsable. Indecd, for such organizations, an argument for becoming a Medicare ACO is that such a commitment enhances their chances for success in commercial global budget contracts. The mote soptisticated potcitial ACOmight also realine that they could grow margin by climinating unnecessary care under capitation, and perhaps earn a hagher percentage of the health care dollar. Insurers, faced with more stringent regulations en MLR's, might be willing to tum some of their cost cutting meastires over to the provsders, wach would fall mto the medical side of the iedger. There will be struggles betweet insurers and providers over responsibilitics for management, and the long-term role of insurers incvitably draws scrutiny in suct relationstips. But many insurers seem committed io trvine ing work out new reimbursement mechanisms. ACO development could also be accelerated by movement from employer-based insurance to the exchange segrent. A state insurance commission-based exchange might conclude that given the limits of cross-subsidy, the need to ensare insurer fiscal stability and the growing costs of coverage, the only solution is to move rapidly out of fee for service and into a prepaid approach. That secms to be the Massachusetts assessment. CMS will likely discern this possibility and bas the wheresithal under the PPACA to develop modets for risk-adjusted capitated payment, using the newly created Center for Innovation. The initial reaction to the new ACO reguations was overwhelmingly negative on the provider side of the ledger, as patients were not "ticd" to the risk-bearing unit, and the upside from management was limited. But that likely does not mean the concept will go away. The real point is, hospitsis and doctors are looking seriously at taking responsibility for population bealth. and they are doing this at least in part because their read is that traditional fee-for-service medicine cannot persist. The question for providers is moving from "whether" to "how." It would appear that insurers and employers are similarty aligned. The Overall Picture In conclusion, the current segment structure of American health care is under a good deal of pressure. The incentives of fee for service have finally broken the federal bank - on that point there is bipartisan agreement - and the limits of employers' ability to pay will mean that cross-subsidies cannot save the day, At the same time, the PPACA's skepticism toward private insuranse mechanisms for reducing costs and lack of commitment to maintenance of lightly regulated self-insured segment appear to be combining with fiscal austerity to create the conditions for changes in the locus of risk for the costs of poot bealth care. Any suck changes in insurance will likely move us toward the accountable care organization concept. Indecd, with an Obarna victory in 2012, we could see care increasingly be provided by ACO's, with risk adjusted capitated payment overseen by insurance commissioners and exchange personnel. The movernents in this direction are incipient, toat there are powerful forces in reform, and in the market, which are impelling us toward a world where providers hold much more risk. Many loosely organized providers in fragmented marketplaces (i.e., much of the U.S.) have difficulty envisioning their path forward, but they know that their current business models coald melt down quickly, Perhaps not in two years, Bill Gates might y, bat almost surely. within ten. The movement to adopt value-based payment (VBP) in the US. health care system tends to focus on getting providers to assume financial risk, Recently, for example, the Centers for Medicare \& Medicaid Services (CMS) finalized its plans to fefilitate the transition to financial risk for providers participating in the Medicare Shared Savings Program. Undet risk-based VBP models, providers are held financially responsible for some, if not all, health care costs if they exceed a predefined budget or a prospectively paid pot of money. In most VBP-rclated work including efforts across commercial, Medicare, and Medicaid payers - there is an underlying goal of moving providers toward risk-based payment models in order to help accomplish the Irinle Aim of better care, lower costs, and healthicr people. National goals for payment reform outlined under the Department of Health and Human Services" Health Cale Bayment Learning. A Dction Notwork fuANi) shift the U.S. toward risk-based payment models including savingsishared risk, bundled payments, and popalation-based payments (see Calcgorie5.3 ant 4 in Exhibit 1). In Medicaid, there are a range of state efforts to "up the ante" on VBP models. For example, six statiz received approval to have their Medicaid payment arrangements qualify as Adyanked Alicmativs Bayment Models under CMS' Quality Payment Program in 2019, which requires a certain level of downside risk. Other states are leveraging initiatives such as Medicadid innosation Simulations and Autyanciog Pramary Catc innoyation in Medicaid Manapelf Cire to design, implement, and ior refine existing VBP models. Exhibit 1: L.AN Payment Reform Gaals Done Its Not Just Risk - Why the Shift t... Medicaid Mathagsd Care to design, implement, and or refine cxisting VBP models. Exhibit 1: LAN Payment Reform Goals Source: Health Care Payment Leaming and Action Network, "ALTERNATIVE PAYMENT MODEL (APM) FRAMEWORK WHITE PAPER: PEFRESHED 2017" July 2017. How Does VBP Financial Risk Impact Providers? Health policy experts talk, about the potential to encourage, gently madge, and in soune cases even force providers "farther to the right" on the LA altemative gaymsmt motel framswork. But, providers are not cmbraciag the shift en masse, and payers have found it challenging to get providers to voluntarily assume financial risk Why is take up slow? Providers are well aware that managing financial risk effectively is expensive and can require additional staff and resources, sach as capital reserves and data systems to manage financial benchmarks. In Medicaid, where providars often operate under rizog-thin margins, the prospect of financial risk can be even more daunting. While risk muly nomica Ponsafial motivatear for providers to stick to a budget and more effectively manage the costs of care, more tessarch is neadat to fully understand how risk impacts individual providers and the amount of risk-bearing needed to produce behavior change. For example, a zaidy of two early adopter Medicaid accountable care organizations (ACO) states - Colorado and Oregon found that Colorado cxhibited a similar reduction in spending without the significant financial risk defining Oregon's model. Other cescarch has shown that financial incentives are generally not passed through from the organizational level to the provider level, meaning that individual physicians are often shielded from any downside risk associated with VBP contracts. Given providers" hesitancy and questions surrounding the impact of financial risk on physician behavior and, ultimately, on the quality and cost of care, what exactly are the benefits of riskbased altemative payment models for providers? Focusing Less on Risk, More an Flexibility How Does VBP Financial Risk Impact Providers? Health policy experts talk, about the potential to encourage, gently makige, and in some cases even force providers " farther to the right +1 on the LAN. alismative paymint model framework, But, providers are not embracing the shift en masse, and payers have found it challenging to get providers to voluntarily assume financial risk. Why is take up slow? Providers are well aware that managing financial risk effectively is expensive and ean require additional staff and resources, such as capital rescrves and data systems to manage financial benchmatks. In Medicaid, where providers often operate under taxor-thin mangins, the prosnect of financial risk can be even more daunting. While tisk may prouide al penverful motivator for providers to stick to a budget and more effectively manage the costs of care, more rithcmeth is nacolat to fully understand how risk impacts individual providers and the amount of risk-bearing needed to produce behavio change. For example, a study of two carly adopter Medicaid accountable care organizations (ACO) states - Colorado and Oregon found that Colorado cxhibited a simitar reduction in spendeng without the significant financial risk defining Oregon's model. Other icscarch has shown that financial incentives are generally not passed through from the organizational level to the provider level, meaning that individual physicians are often shielded froen any downside risk associated with VBP contracts. Givea providers" hesitancy and questions surrounding the imapact of financial risk on physician behavior and, ultimately, on the quality and cost of care, what exactly are the benefits of riskbased alternative payment models for providers? Focusing Less on Risk, More on Flexibitity Some health policy experis have made a pompelling carse that the shift to VBP is not really about risk, but about frexibility namely, the financial flexibility to provide the light cilts in the tight place at the rielt time. The fee-for-service payment system is problematic not just because of its inherent incentives to increase the volume of services provided without regard for quality or cost. It also limits the care that providers gencrally deliver to those services that have an associated payment code. The fce-for-service payment system reimburses for services covered under a payer's fee schedule, but does not typically reimburse for things that could help avoid an office or cmergency department visit, Ush as respent tint to puticnt phons sors mantage to belp patients with chronic conditions, or addressing patients' sosialsktermitants of health. Further, fee schedules typically limit where services can be provided (often limiting the place of service to a provider's office) as well as who can provide services (often to the exclusion of highvalue, culturally adept providers, such as conntriuatity herlth Wwikers and pace providers). Newer fee-for-service codes sach as those for certain types of hehavional health intsgration and iclshealth services in Medicare do offer reimbursement for expanded types of services relative to traditional office-based codes; however, adding new billing options code-by-code and payer-by-payer is a cumbersome way to keep pace with innovation, as evidenced by the limitcd upiahe of these new codes to date. Altemative payment models, such as population-based payments, provide broader flexibility in where, how, and by whom care is delivered, and inherently involve some risk. While this risk is a necessary by-product of changing from a fee-for-service hased payment system to one that allows for more flexibility, it may be better viewed as a means to an end: the " hility to inaprove Examples of VBP Supporting Flexibility and Care Transformation A perfect example of this need for flexible dollars to support care transformation is illustrated by Somthoentril Foundation, a health care provider for Native Alaskans in Anchoragc, Alaska. Southeentral has integrated treatment for mental healih inte its primary care practices, and found that paticnt aitisfaction mites skyrocketed, while the use of medical care went down. As a. result, Southeentral has been a victim of tis own success because patients in its integrated practices needed less medical care, the doctors mate less moncy. This canundrum is not unique to Southcentral. A study of integrated team-based care approaches found that integrated practices generate $115 per patient less annually, on average, than traditional fee-for-service payment methods. This means that, from a business perspective, provider practices confront financial disincentives for integrating care unless the payment model is changed to incentivize kecping patients healthy - something that population-based payments are well-equipped to do, A number of states, including Conncelisil and Rhoulc Island have promoted the virtues of flexibility in new VBP models, particularly in primary care. Rhode Island's Office of the Health Insurance Commissioner (OHIC) Primary Care Alternative Payment model is a capitated approach designed to achieve better care, smarter spenditig. and healthier people by supporting primary care providers' use of "'flexible approaches to communication, monitoring, and treatment. "Notably, OHIC states that providers of any size can suceeed under a capitated arrangement, and clarifies that the goal of the model is not to reduce primary care spending or to shift insurance risk to primary care providers. Designing population-based payment models that can apply to smaller providers is cracial given that practices with only one of two physicians have demonstrated the ability to provide high-quality, cost-effective care. Chris Koller, President of Milbank Mernorial Fund, recently highlighted syidencs demonstrating that "practices with just one payment meinous. 1 ms means tmal, atom a ousiness perspectue. provider practices confront financtal disincentrves for integrating care unless the payment model is changed to incentivize keeping patients healthy - something that population-based payments are well-cquipped to do. A number of states, including Comncelisul and Rhods leland have pro4noted the virtues of flexibility in new VBP models, particularly in primary care. Rhode Island's Office of the Health Insurance Commissioner (OHIC) Primary Care Altemative Payment model is a capitated approach designed to achieve better care, smarter spending, and healthier people by supporting primary care providers' use of "flexible approaches to communication, monitoring, and treatment." Notably, OHlC. states that providers of any size can succeed under a capitated arrangement, and clarifies that the goal of the model is not to reduce primary care spending or to shift insurance risk to primary care providers, Designing population-based payment models that can apply to smaller providers is cracial given that practices with only one or two physicians have demonstrated the ability to provide high-quality, cost-effective care. Chris Koller, President of Milbank Memorial Fund, recently highlighted syidcnce demonstrating that "practices with just one of two physicians produced oulcort ics that were as good as those of their larger siblings and significantly better than practices with over 100 physicians." Likewise, Conthacicut is developing a new primary care bundled payment model that aims to provide practices with "true flexibility" by providing upfront payments to cover the time the care team spends doing traditionally unfunded or under-fursded work such as bome visits, telemedicine visits, and phone, c-mail or text support. Looking Ahead Moving forward, the drive toward VBP and risk-based payment models is likely to continue, with Medicaid leading the way in some cases. For example, comrunity health centers and other afety net providers consider Medicaid and new opportunities around VBP to be the motepromising fintuse \#mitse of Leyerius for expanding their efforts related to social determinants of health. CMS is also cmphasizing greaty flex thility for providers and states, a willingness to test state-based and local models, and an interest in provider-led innovation. As the VBP joumey continues, it may be worth focusing more directly on the move toward increased financial fleribifity fot providers that certain risk-based VBP models allow (and, consequently, on true payment reform that moves away from payment models built upon fee-for-service architecture), instead of on their increased financial wisk