

Question: After reading the case study attach below , must reference material in the reading assignment What reimbursement method would you recommend for each of the
After reading the case study attach below , must reference material in the reading assignment
- What reimbursement method would you recommend for each of the following providers (Primary Care Physicians; Specialists; Hospital and Other services)? Justify your answers.
- What allocation of premium dollars do you recommend for each provider? Justify your recommendations.
- Should all the physician hospital organization's (PHO) physicians participate in the contract, or should subpanels be formed?

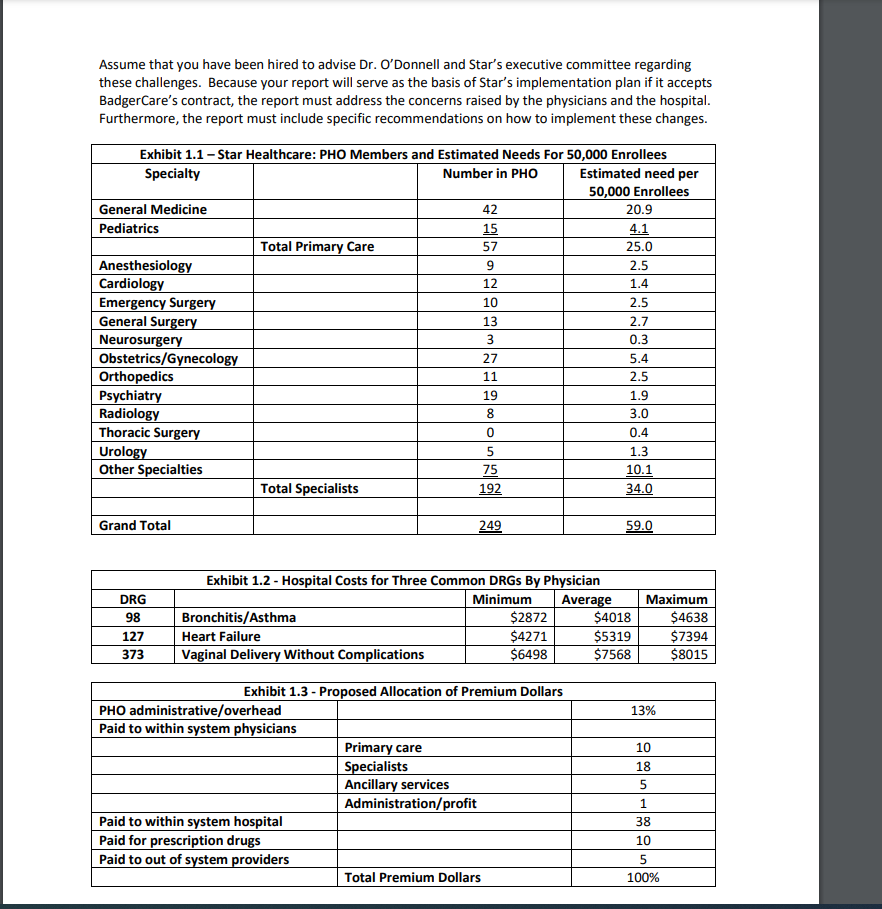
Star Healthcare: Capitatian and Risk Sharing Star Healthcare is a community hospital in Green Bay, Wisconsin. Recently, the hospital and its affiliated physicians formed Star Memorial Hospital, a physician-hospital organization {PHD}. Star is close to signing its first contract to provide exclusive local healthcare services to enrollees in BadgerCare {the planl, the local Blue Cross Blue Shield of Wisconsin HMD. For the past several years, the Plan has contracted with a different Green Bay PH D, but nancial difculties at that organization have prompted the plan to consider Star as an alternative. In the proposed contract, Star will assume full risk for patient utilization. In fact, the proposal calls for the PHD to receive a xed premium of $200 per member per month from the Plan, which is then can allocate to each provider component in any way teams best using any reimbursement method it chooses. Star's executive director, Dr. George D'Donnell, a cardiologist at a recent graduate of the University of Wisconsin Non-resident Program in Administrative Medicine, is evaluating the Plan's proposal. To help to this, Dr. O'Donnell hired a consulting firm that specializes in PHD contracting. The first task of the consulting firm was to review Star's current medical panel and estimate the number of physicians, by specialty, required to support the Plan's patient population of 50,000, assuming aggressive utilization management. The results in exhibit 1.1 show that Star's medical panel consists of 249 physicians, whereas the number of physicians required to support the Plan's patient population is only 59. Note, however, that Star's physicians serve patients other than those in the Plan. Thus, the total number of physicians required to treat all of Star's patients far exceeds the 59 sh own in the right column of the table. The second task of a consulting firm was to analyze Sta r's physicians' current practice patterns. Clearly, utilization, and hence cost, is driven by Star's physicians and that variation in practice patterns is costly to Star. Results of the analysis show significant variation in practice patterns, both in physician's offices and in the hospital. For example, exhibit 12 contains summary data on hospital costs by physician for three common diagnosis-related groups [DRGs]. Consider D516 12? {heart failure}. The physician with the lowest hospital costs averaged 54,221 in costs per patient, the highest cost physician averaged 52,3 94, and the average cost for all physicians was $5,319. The consulting firm commented that reducing this variation is important because Star is at full risk for patient utilization. The third task of the consulting firm was to recommend an appropriate allocation of the premium dollars to each category of provide r. Specically, the con tract calls for Star to receive $200 per member per month, for a total annual revenue of 5200 x 50,000 members x 12 months : $120,000,000. To reduce potential conflicts about how to divide the $120,000,000 among providers, the consulting firm proposed a \"status quo" allocation that would maintain current revenue distribution percentages shown in exhibit 1.3. Final task of the consulting firm was to recommend provider reimbursement methodologies that create appropriate incentives. In the contract, Star assumes full risk for patient utilization, so the consulting rm recommended that all component providers be capitated to align cost minimization incentives across throughout Star. Furthermore, capitation of all providers would eliminate the need for risk pools, and risk sharing arrangement that Star has never used. In addition to the consulting firm's report, Dr. D'Don nell decided to ask Sta r's new operations committee for a short report on the current line of thinking among Star's major providers. The committee provided the following information. Star Healthcare Historically, the profitability of Star Healthcare has been roughly in line with the industry. Last year, when the hospital received about 15% of charges, on average, the hospital achieved an operating margin of about 3%. However, hospital managers are concerned about its profitability if the Plan's proposal is accepted. The managers believe that controlling costs under the full-risk contract would require extraordinary efforts and the most effective wat to control costs is to create a subpanel of physicians to participate in the capitation contract. when asked how the subpanel should be chosen, the operations committee recommended choosing physicians would do the best job of containing hospital costs. Primary Care Physicians Many ofthe primary care physicians are dissatised. On average, primary care physicians receive only about 50% of charges and are concerned about being penalized by accepting utilization risk for the Plan's enrollees. Primary care physicians know they are paid less and believe they must work much harder than do the specialists. Furthermore, primary care physicians believe that the specialists supplement their own incomes by over using in office tests and procedures. Some primary care physicians are even talking about dropping out Star to form their own contracting group, taking away the entire capitation payment from the Plan and contracting themselves for specialist and hospital services. Specialist Care Physicians The specialists believe that the primary care physicians refer to many patients to them. The specialists do not mind the referrals if their reimbursement is based on charges because, on average, they receive 90% of charges. However, if they are capitated, the specialists want to primary care physicians to handle mo re of the minor patient problems themselves. Also, whenever the subject of subpanels is raised, many of the specialists become incensed. r\"miter all,\" they say, "the whole idea behind the PHD is to protect the specialists." Both sets of physicians - primary care and specialist - agree that the hospital is hopelessly inefficient. Said one specialist, r\"No matter how much revenue the hospital receives, it still seems to barely make a profit." To respond to the Plan's proposal, Dr. D'Donnell and Star's executive committee must decide whether to accept the recommendations of the consulting firm. Specifically, these questions must be addressed: 1. What proportion of the expected 52cm per member per month capitation payment from the Plan should be allocated to each component {for example, hospital, primary care physicians, specialists, and other providers]? 2. Are risk pools necessary? If so, what other incentives should be put in place to control utilization? 3. What payment method should be used for each provider? Should all providers be capitated?I Anybody capitated? Should some combination ofthese methods be used? 4. Should all of Star's PHD physicians participate in the contract, or should subpanels be formed? If subpan els are formed, how should they be constituted? 5. What other actions should Star undertake to successfully manage this full risk contract? Assume that you have been hired to advise Dr. O'Donnell and Star's executive committee regarding these challenges. Because your report will serve as the basis of Star's implementation plan if it accepts BadgerCare's contract the report must address the concerns raised by the physicians and the hospital. Furthermore, the report must include specific recommendations on how to implement these changes. Exhibit 1.1 -Star Healthcare: PHD Members and Estimated Needs For 50,000 Enrollees Specialty Number in PHD Estimated need per 50,000 Enrollees General Medicine 42 20.9 Pediatrics g Q Total Primary Care 5'." 25.0 Anesthesiology 9 2.5 Cardiology 12 1.4 Emergency Surgery 10 2.5 General Surgery 13 2.? Neurosurgery 3 0.3 Dhstetricstynecology 2'." 5.4 Orthopedics 1 1 2.5 Psychiatry 19 1.9 Radiology 3 3.0 Thoracic Surgery 0 0.4 Urology 5 1.3 Other Specialties E 10_.1 Total Specialists Q E Grand Total a m Exhibit 1.2 Hospital Costs for Three Common DRGs By Physician DRG Minimum Average Maximum 98 Bronchitis} Asthma $2822 $4013 $4633 12? Heart Failure $4221 $5319 $2394 323 Vaginal Delivery Without Complications $6498 $2553 $8015 Exhibit 1.3 Proposed Allocation of Premium Dollars PHD administrativefoverhead 13% Paid to within system physicians Primary care 10 S ecialists 18 Ancillary services 5 Ad ministrationfprofit 1 Paid to within system hospital 38 Paid for prescription drugs 10 Paid to out of s stern roviders 5 Total Premium Dollars 100%
Step by Step Solution
There are 3 Steps involved in it

Get step-by-step solutions from verified subject matter experts