Question: HAD509 Written Case Analysis Content and Format (Adapted from: Simendinger, E. (2003). In Search of a Course Design and Teaching Methods to Improve Critical Thinking.
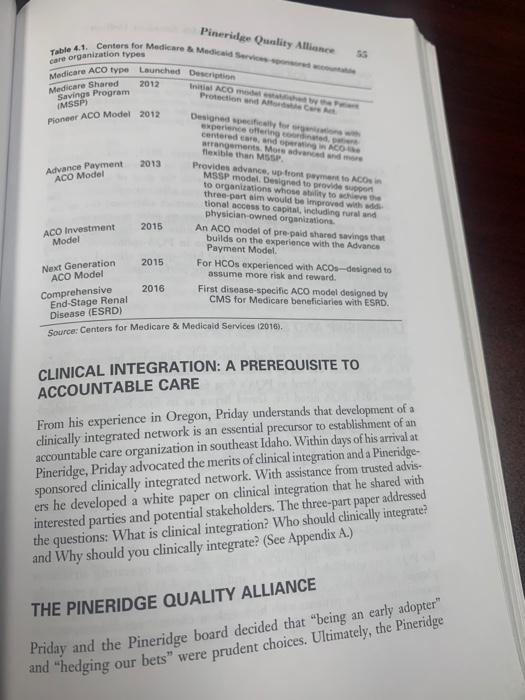
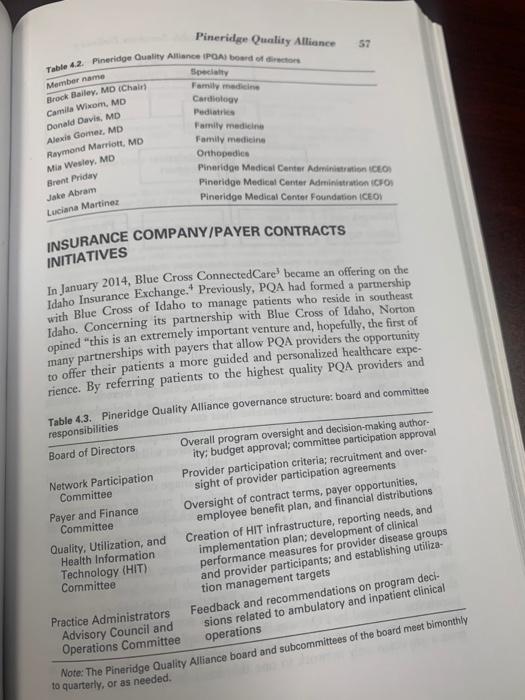
HAD509 Written Case Analysis Content and Format (Adapted from: Simendinger, E. (2003). In Search of a Course Design and Teaching Methods to Improve Critical Thinking. Journal of Health Administration Education, 20(3), 197-213.) Do each case analysis without discussing it with other HAD 509 students prior to the due date. For each case, write the following information and number it 1 though 8 and use section headings: 1. Your name 2. The case number, case title, and class date. 3. 4. A summary of the case. [1 paragraph) This will require you to read the case several times. Do not just copy sentences from the case. Instead, express in your own words the essence of the case. A list of what you think are the 10-15 most important facts/factors in the case [1-2 pages). I page The most important health administration problem/issue to be solved in the case. [1 sentence]. 1 page List other secondary problems in the case [1-2 pages). 5. 6. Your recommended solution for the case (a.-d. below). Make clear specific realistic recommendations. There must be a clear logical sequence to your thoughts and recommendations. [4- 5 pages) a. At least three possible realistic alternative solutions for the most important problem (stated above for 5). b. Criteria to evaluate possible alternative solutions. For example: acceptability to stakeholders, needed resources, legality, timing, cost-effectiveness, ability to implement, side effects, qualifications, statistical data, financial data, ethical considerations, fit with case facts, likelihood of actually solving the problem, etc. c. Evaluation of the possible alternative solutions (6a) using the criteria (6b). d. Your recommended solution for the problem, based on 6a, 6b, and 6c. Justify your recommendation. 7. Specific MHA tools, methods, techniques, principles, theories, models, etc. from MHA courses that you used for this case. List specific tools (e.g., cost-benefit analysis, market segmentation, etc.). Do not list general subjects (e.g., finance, leadership) [1-2 pages]. 8. Answer any case study questions that accompany the case. If a case question is answered by what you already wrote for 3-7 above, then just note which part of your case analysis provides the answer. Submit your written reports by 11:55 pm on the Sunday of each week. chew A Case Study in Clinical Integration Pineridge Quality Alliance is a study in clinical integration, accountable care organizations, and population health. The case study profiles the his- . AIDS chase Merck .Org rek's Pineridge Quality Alliance be com of and Population CASE HISTORY/BACKGROUND tory, challenges , and opportunities related to development of a clinically integrated network and the sponsoring organization's quest to become an accountable care organization and engage in population health. In June, 2012, Brent Priday arrived in Pocatello, Idaho, as the newly appointed CEO of the 187-bed Pineridge Medical Center (Pineridge), which had been established in 2002 following the consolidation of Pocatello's two regional hospitals. Priday had served previously as CEO of West Valley Medical Center in Harrisburg, Oregon, where his 120-bed hospital participated in a "coordinated care organizationla new state- sponsored healthcare delivery model that seeks to lower costs and improve quality for Oregon Medicaid patients. Priday is convinced that coordi- nated care organizations and their variants are the wave of the future, and that Pineridge had to get onboard. 53 Policy Environment of Health Services Delivery Care Act in 2010 (U.S. Department of Health and Human Services, 2015) Priday believes that passage of the Patient Protection and Nicole healthcare business model, including reimbursement reductions, provides transforming the traditional from a Curve I (volume-based) to Curve 2 (value-based) paradigan (unes recapitalization and reconfiguration, and new payment models Though the pace of change will vary by market, Priday believes the readiness. The question looming for Priday and the Pineridge board is shift from Curve I to Curve 2 will happen irrespective of an organization's Wait and see: Maximize fee-for-service opportunities until the market 54 is a catalyst for disruptive forces that are & Gursahaney, 2014), Which of three common approaches should Pineridge take? . requires a shift or creates sufficient financial upside to do so. Be an early adopter. Create first-mover advantage by creating an accountable care organization/clinically integrated network to offset the impact of reduced reimbursement and utilization by increas ing market share of covered lives and keeping more of the services delivered to those living within our network. Hedge our bets: Experiment with pay-for-performance contracts and manage our health system's employee populations until more drastic change is warranted (Butts & Gursahaney, 2014). Since passage of the Affordable Care Act, over 750 accountable care organi- zations have been formed nationwide.? In advancing the concept of account- able care and the merits of clinical integration, Priday explained to Pineridge Medical Center's board of trustees that accountable care organizations are basically groups of doctors, hospitals, and other healthcare providers who organize voluntarily to give coordinated, high-quality care to Medicare and other patients. Coordinated care helps ensure that patients, especially the chronically ill get the right care, in the right place, at the right time, with the goal of avoiding unnecessary duplication of services and preventing medical errors. Priday noted that when an accountable care organization succeeds in both delivering high-quality care and spending healthcare dollars more wisely, it will share the savings it achieves for the Medicare program (Center for Medicare and Medicaid Services: Accountable Care Organizations, 2016). Priday knows his organization is not ready to form an accountable care organization per se and participate in accountable care organization pro- grams with the Centers for Medicare & Medicaid Services. Nevertheless, he understands the different kinds and types of accountable care organizations and is preparing his organization for eventual participation. A sample of accountable care organization programs sponsored by the Centers for Medicare & Medicaid Services is outlined in Table 4.1. Table 4.1. Centers for Medicare & Media Servo Medicare ACO type Launched Description Pinerilge Quality Alliance 2012 Initial ACO med Protection and A Medicare Shared Savings Program IMSSP) Pioneer ACO Model 2012 2013 Advance Payment ACO Model Designed specify for experience offering con centered care and AO arrangements Mots advanced texible than MSSP. Provides advance up front payment to ACOS MSSP model Designed to provide support to organizations whose wity to where the three-port im would be improved with a tional access to capital, including rural and physician-owned organisations An ACO model of prepaid shared savings that builds on the experience with the Advance Payment Model For HCOs experienced with ACOs-designed to assume more risk and reward. First disease-specific ACO model designed by CMS for Medicare beneficiaries with ESRD. 2015 ACO Investment Model 2015 Next Generation ACO Model Comprehensive End-Stage Renal Disease (ESRD) 2016 Source: Centers for Medicare & Medical Services (2016). CLINICAL INTEGRATION: A PREREQUISITE TO ACCOUNTABLE CARE From his experience in Oregon, Priday understands that development of a clinically integrated network is an essential precursor to establishment of an accountable care organization in southeast Idaho. Within days of his arrival at Pineridge, Priday advocated the merits of clinical integration and a Pineridge- sponsored clinically integrated network. With assistance from trusted advis- ers he developed a white paper on clinical integration that he shared with interested parties and potential stakeholders. The three-part paper addressed the questions: What is clinical integration? Who should clinically integrate? and Why should you clinically integrate? (See Appendix A.) THE PINERIDGE QUALITY ALLIANCE Priday and the Pineridge board decided that "being an early adopter" and "hedging our bets" were prudent choices. Ultimately, the Pineridge Policy Environment of Health Service Delivery Oy Alliance (POAclinically integrated network the bing higher increased teen themen contracts were extended to clinicians initially in Bannock and the Concurrent with its launch in late summer 2013, initial counties (POA's primary service area) with the goal of extending invitation to hospitals and clinicians in seven adjacent counties over next 12-36 months (Appendix B). POA contract addressed the folle ing key provisions: the need for transparency: joint contracting with insurance plans compliance with PQA initiatives including adher. ence to clinical benchmarks, participation in PQA-sponsored training and agreements to track and share quality performance measures and programs, and adoption of efficient and high-quality clinical practice dren of the dishes and their lider 56 in August 2013. POA has the following mission To be there am deste Table 4.2 Pinerid Momber name Brock Bailey, MD Camila Winom, M Donald Davis, ME Al Gomez, Raymond Marri Mia Wesley M Brand Priday J Abram Luciana Mart POA and December 19, 2011) INSURA INITIAT other data In Januar Idaho Ir with BB: Idaho. opined many to off rience Table respo Boa Net Pa LEADERSHIP AND STRUCTURE In the months leading up to and immediately following initiation of the PQA, the alliance was led by an external consultant. In September 2014, Karlyn Norton was hired as PQA's first full-time executive director. In August 2015, PQA hired Dr. David Bryan as its first full-time medical director. Bryan noted, "Pineridge Quality Alliance is the first and only clinically integrated network in eastern Idaho. It was founded and is oper- ated by physicians in the interest of improving quality and controlling the cost of medical care using robust and accurate data. It is clearly the future of medical care." Since its inception, PQA has been a physician-led organization, with a 9-person board of directors, 6 of whom are physicians (Table 4.2). In December 2013, the PQA governance structure was formed (Table 4.3). By mid-2014 the foundational governance and operating structures for POA were established (Table 4.3 and Figure. 4.1). Norton is especially pleased with the July, 2015, hiring of two full-time "care managers who coordinate care for patients with high-risk or chronic conditions , or who simply need someone to help them navigate the complicated healthcare system. INSURANCE COMPANY/PAYER CONTRACTS Table 4.2. Pineridge Ouality Alliance IPOAI board of director Pineridge Quality Alliance 57 Specialty Family medicine Cardiology Pediatrie Family medicine Family medicine Orthopedice Pinnridge Medical Center Administration CEO Pineridge Medical Center Administration ICFO Pineridge Medical Center Foundation ICEOX Member name Brock Bailey, MD (Chairs Camila Wicom, MD Donald Davis, MD Alexis Gomez, MD Raymond Marriott MD Mis Wesley, MD Brent Priday Jake Abram Luciana Martinez INITIATIVES In January 2014, Blue Cross ConnectedCare? became an offering on the Idaho Insurance Exchange. Previously, PQA had formed a partnership with Blue Cross of Idaho to manage patients who reside in southeast Idaho. Concerning its partnership with Blue Cross of Idaho, Norton opined "this is an extremely important venture and hopefully, the first of many partnerships with payers that allow PQA providers the opportunity to offer their patients a more guided and personalized healthcare expe- rience. By referring patients to the highest quality PQA providers and Table 4.3. Pineridge Quality Alliance governance structure: board and committee responsibilities Board of Directors Overall program oversight and decision-making author ity; budget approval committee participation approval Network Participation Provider participation criteria: recruitment and over- Committee sight of provider participation agreements Payer and Finance Oversight of contract terms, payer opportunities. Committee employee benefit plan, and financial distributions Quality, Utilization, and Creation of HIT infrastructure, reporting needs, and Health Information implementation plan; development of clinical Technology (HIT) performance measures for provider disease groups Committee and provider participants; and establishing utiliza- tion management targets Practice Administrators Feedback and recommendations on program deci- Advisory Council and sions related to ambulatory and inpatient clinical Operations Committee operations to quarterly, or as needed. Note: The Pineridge Quality Alliance board and subcommittees of the board meet bimonthly In July 2016, Norton explained that drastic changes were being made further incentivize patients to receive their care within the PQA network. . Piner partners Blue Cros Care POA and of Director 2014 PMC EC thro Blue n. 2015 Jan 2015 Ro the opportunity to more actively participate in their patients' downstream se. Only then will the alliance begin to coordinate care better, reduce newry procedures, and improve overall health status of those they Pharmacy management providers Analytics support July 2015 Ipport Credentialing Care Human Pineridge Qual A point maintenance HMO, partici a PPO, 2. UMA administra services 3.A certain management Mually Alliance, table of organisation care enti Berlying them navigate their services, PQA enables primary pro PC NE Going forward, the added copay and deductibles to patients who opt out of PQA will be so significant that far fewer services will be sought outside the network. The shift in plan design will reinforce the importance of staying in the network and allowing PQA to manage care more effectively than could be done with traditional preferred provider organization plans. In early 2015 PQA extended its relationship with Blue Cross of Idaho to support True Blue Medicare Advantage members in southeast Idaho, thus enabling PQA to perform population health and care man- agement activities for these more resource-intensive, difficult-to-manage Medicare patients. In mid-2015 PQA contracted with Regence BlueShield of Idaho on that insurer's Total Cost of Care program in southeast Idaho. Another population managed by PQA was Pineridge employees and their depen- dents (effective January 2015). This arrangement required an expansion from a physician-only network to one that included providers across the administrator. Founded in 1983 as United Medical Resources, UMA provides administrative allied health specialties (Table 4.5). The PQA network growth by selected Pineridge Quality Alliance Pineridge Quality Alliance partnership Table 4.4 Population health contract initiatives Non Humana, Pacific Source, and Aetna have expressed interest in partnering with maintenance organization (HMO) and preferred provider organization (PPO) plans. Like MMO participants designate an in-network physician to be their primary care provider. But 59 Summary Commercial point of vice Blue Cross of Idaho Connected Population estimate 1.700 members Commercial third party admin trator Population state 2.300 members Medicare Advantage henkman tenance organization. Population estimate 900 members Commercial preferred provider organization. Population et mate: 700 members. Dute Jan. 2014 Care PMC Employee Health Plan through UMRO Jan 2015 Blue Cross of Idaho True Blue Jart, 2015 Regence Blue Shield of Idaho Total Cost of Care July 2015 Pineridge Quality Alliance WaPpo. patients may go outside of the provider network for healthcare services services for self-funded health insurance plans. . A third-party administrator (TPA) is an organization that processes insurance claims or certain aspects of employee benefit plans for a separate entity entire continuum of care, including allied and ancillary professionals/ providers (see Table 4.4), thus allowing the provider network to sup- port the employee health plan's third-party administrator (UMR (United Medical Resources]). Norton said the hospital is interested in using its new clinically integrated network to prove it could deliver better quality care for employees at lower overall cost. A summary of these population health-related contracting initiatives is provided in Table 4.4. NETWORK DEVELOPMENT AND GROWTH Two years following inception, PQA included 580 clinicians from 7 provider groups representing not-for-profit, for-profit, public, private, urban, and rural-based domains all working toward a common goal of clinical transformation and collaboration consistent with the Institute for Healthcare Improvement Triple Aim. By fall 2016, PQA included representation from over 30 medical and specialties is outlined in Table 4.6. Policy Environment of Health Services Delivery Table 45 Pineridge Quality Alliance network and specialty composition they don 60 Otorhinolaryngology Pediatrics Home het Hospice in a clinically the POA fee sch of PQA-insuran critical access hac POA: she unde will be limited grated network Anesthesia Ambulatory surgery center Behavioral health Physicalloccupational speech therapy Podiatry Psychiatry Psychology Independent lab Internal medicine Nephrology Neurology CLINICAL TOOLS-P Cardiology Chiropractic Durable medical equipment Endocrinology Family practice Gastroenterology Obstetrics bynecology Ophthalmology Optometry Pulmonology Radiology Skilled nursing facilityong term acute care unit Urgent care Urology Not surpris by early 20 clinically tice manag Orthopedics General surgery tools kno firm (Ad- Davis ex observir The PQA was relatively successful in recruiting participation from physicians and allied health professionals in Bannock County, but by early 2016 the alliance had been unable to secure contracts with surrounding critical access hospitals and clinicians in southeast Idaho (Appendix B, District 6). Norton explains that these rural, independent hospitals and their local physicians do not feel any urgency to change. She also believes have me exist, a collect Advan Table Hel and cie Table 4.6. Pineridge Quality Alliance network growth by selected specialties 2014 2015 2016 Provider types 185 213 240 Family practice 12 13 17 Internal medicine 8 9 9 Pediatrics 12 Obstetrics/gynecology 12 12 14 Orthopedics 16 16 Cardiology 16 25 25 General surgery 7 7 Behavioral health 33 Chiropractic Physical occupational/speech therapy 111 133 Home health/hospice 9 16 Other 408 492 45 5 135 16 527 in a clinically integrated network. Some base they don't fully understand the purpose of the POA fee schedule) to care for patients they were of POA-insurance company contracts, North POA: she understands that without a reader en PON will be limited in its ability to fully realize the nefits in critical acces hospitals in the regionsresowe grated network (see Appendix A. Why should yodinically Nor surprisingly, the more than 70 organizations that made up the POA tice management systems. To facilitate realization of the benefits of a truly by early 2014 employed many kinds and types of medical records and clinically integrated delivery system, in mid-2014 PQA purchased a set of firm (Advisory Board Company, 2016). PQA board member Dr. Donald rools known as Crimson from the Advisory Board Company, a consulting Davis explains that Crimson "will allow us to start collecting data and observing quality measures from all providers in the network. Once we have meaningful data we can decide where there is variation, why outliers exist, and how we can implement strategies to improve our individual and TOOLS-PROGRAMS-SERVICES collective outcomes. The three modules that make up Crimson Clinical Pineridge Quality Alliance CLINICAL INTEGRATION Advantage are outlined in Table 4.7. Table 4.7. Crimson Clinical Advantage Crimson Continuum of Care Helps hospitals achieve the physician alignment needed to advance quality goals and secure cost savings. Places credible performance profiles in the hands of physi- cians, enabling them to better meet healthcare organization cost and quality goals. Crimson Population Risk Management Helps hospitals manage total cost and quality for defined populations including self-insured employee plans-and inform risk-based contract negotiations with payers. Combines insight on health system strategy with a robust benchmarking database and clinical algorithms; physicians get a 360-degree view of patient care, including an evaluation of the organization's strengths and liabilities, and more. Crimson Care Management Helps hospitals create and run effective, collaborative care management programs by providing intelligent workflows and integrating complex data sources to custom- ize care programs and drive compliance. Generates data that will unlock actionable insights that help care managers work smarter and maximize impact. network with access to powerful data is that we start to pay attention to our patients overall health, no matter where they receive the together as a collective team to provide the highest quality care, WW care, because we now have visible data. And, because we are now working the entire network of PQA providers to do well, not just ourselves Concerning Crimson Care Management, Norton notes that Crim reams. Crimson generates to-do tasks, alerts, and reminders in response to analyzes data fast enough to provide real-time updates to patient care patient admission, discharge, or care program data. It then routes action as needed. The Crimson Population Risk Management tool can easily requests to the appropriate care team members for prompt intervention, track member, population, and provider progress toward organizational clinically integrated Davis explains that one important benefit to a truck bor Additions to practic problems provided CLINI In con Policy Environment of Health Services Delivery and contractual goals. In elaborating the merits of clinical integration and the need for population health and care management, Norton often uses Figure 4.2 as an example of how the Crimson software categorizes populations into high-risk, rising-risk, and low-risk care categories. Once the population is risk stratified, providers can focus on persons who need the most help. Norton further explains that Crimson software integrates data from patient registries, electronic health records, and other practice management systems to improve coordination of care delivery between and among primary and special practices and hospitals. Since 2014, PQA has implemented the capabilities of Crimson Continuum of Care at each physician site, enabling these providers to provid perfos tinec Systet and to be exp Qu (Ar +8 E Meet Your Three Patient Populations HIGH PATIENT COMPLEXITY DRIVING OUTSIZED PATIENT COSTS... ..REQUIRES CREATING THREE UNIQUE PATIENT POPULATIONS WITH THREE COMPLEMENTARY CARE MODELS PERCENTAGE OF MEDICARE BENEFICIARIES HIGH-RISK SW OF POPULATION PERCENTAGE OF TOTAL MEDICARE SPENDING RISING RISK 20% OF POPULATION LOW RISK 754 OF POPULATION MM OF CONCTIONS HOORONE ho ME SOKOR MORE Figure 4.2. Crimson Capabilities (Advisory Board Company, 2016). track both aggregate and patient-specific clinical and final data Additionally, POA staff provides agregate and peactice-pecific reports problems represent opportunities for improvement. Sample reports to practices and selected PQA committees. Provider and patient-specific CLINICAL AND OPERATIONAL MEASURES In conformance with the POA Participating Provider Ngreement, POA performance improvement and data-sharing initiatives to share data con providers agree to actively and meaningfully participate in the alliance's trined in medical records, billing, claims, practice management, or other systems, clectronic, or otherwise. In fall 2014, the PQA Quality, Utilization, Pineridge Quality Alliance in and HIT committee, with approval of the PQA board, selected 15 measures to begin tracking and analyzing. Donald Davis, a pediatrician on the board, explains "These are Physician Quality Reporting System and National (Appendix D). In 2015, PQA legal counsel recommended the alliance add 48 more measures: 5-10 per major provider type for a total of 63 measures. EDUCATION AND TRAINING In November 2014, PQA leaders announced it would collaborate with Optum" to provide a series of educational opportunities focused on the Medicare Advantage Risk Adjusted Program and the Medicare Access and CHIP Reauthorization Act of 2015. Norton reported the following: Optum works with healthcare professionals and health plans to help them attain improved health outcomes. With relevant tools and support, Optum can help healthcare providers in the early detection, ongoing assessment, and accurate reporting of chronic conditions. ... Optum has technology and health intelligence solutions that help providers accu- rately document and code conditions while improving the overall quality of care.... The investment in technology, education, and training is key to PQA's ability to achieve the noted "Triple Aim." Buck Ridley, PQA's information technology specialist, observed in the first year (following implementation of the Crimson and Optum initia- tives) "we will be able to see, individually and collectively as an alliance, where the opportunities for improvement are. By year 5, we will use the information in a sophisticated manner to improve the overall cost, quality, and utilization of care we deliver." community to improve quality and reduce costs of care for their emplo ces. Additional quality measures, clinical pathways, and care management At the June 2016, PQA board retreat Priday addressed the following . Succeeding in population health requires more than completing a either due to their insufficient payer capabilities or limited geographic 6-4 POA works in o rurality, We don't h have. Thu our comm allow our need with Policy Environment of Health Seri Delivery LOOKING BACK LOOKING AHEAD Reminiscing three years following is inexp. PCROP observed. We wanted to create profil hanged patient care that will directly affect the health of time in which our industry has been turned on its head rem it limits, we have intimated transformation that will repite even mere from us than has already been dered Three years following is loch, POA has invested renghly $2.5 million administrators and clinicians have invested well in excess of 2016 in planning and implementation related activities. The future include ships, working with Human regarding opportunities for their Medicar Advantage members, partnering with Aetna on their commercial The ger our pro and que consun differs that we Alth thes cian thes sti th Inf pli ne pe . programs represent other opportunities for developing improvement challenges common to the industry: Medicare Shared Savings Program application and creating a Federal Trade Commission-compliant structure. Creating an effective and scalable population health/clinical integra- tion infrastructure requires a significant investment of capital, time and resources. It is extremely difficult to align providers across the care continuum in a way that drives quality and sufficient cost savings to create meaningful shared savings dollars. The financial benefits of shared savings programs are directed at poi mary care physicians and are inherently short term unless they incor porate bundled payments as a means to engage specialists and focus on reducing spending on high-cost procedures. Payers are often unwilling to structure mutually beneficial contracts with networks that offer sufficient upside potential to offset losse in fee-for-service revenue because the networks have unproven track records or lack sufficient geographic reach to meet access requirements. Not all networks are capable of contracting directly with employers coverage for a broad employee base. challenges specific to POA: In the context of these industry-wide ises, Norton disco POA has unique challenges compared with dinically integrated works in other parts of the county due to i topography We don't have the span of providers and specialties that makes our community to form lasting and collaborative partnerships that will have. Thus it's critical for us to all with independent power allow our patient populations to access the high-value services they The geographic, rural, and relatively sparsely populated nature of our provider community means we must strive for excellence in con and quality and to have an accurate measure of what the healthcare consumer perceives as "value" because their definition may be quite different from ours. As consumers become more savvy. we must ensure that what we offer meets their expectations. . Although PQA board members publicly affirm their commitment to their practices is difficult. One prominent board member privately successfully navigate the transition from Curve I to Curve 2" (Butts & Pineridge Quality Alliance rurality leaving . . the clinically integrated network, getting those leaders and other physi- stated, "Honestly, I'm not sure I get it. Crimson is complex and I'm still not using the data to change or improve my practice." Even though the PQA medical director is talented and committed to the cause, he is stretched too thin and unable to meet with network physicians and clinicians to teach, motivate, or monitor their performance, In frustration, Norton occasionally reaches out to a seasoned and accom- plished mentor from across the state. "Look" the mentor said, your network is new and small, but look at what you have accomplished...be patient, learn to fail 'as fast and inexpensively as possible'... and just keep moving forward!" Priday and Norton say their observations/conclusions should not lead PQA to abandon its clinically integrated network and eventual account- able care organization strategy because pressure from employers to reduce premiums and the government's expansion of value-based programs will continue, regardless. Rather, they contend, "If we are going to be paid differently, we must organize and deliver care in a way that leads to dif- ferent results. Developing our clinically integrated network is a way for us to respond to these changes, overcome the above challenges , and achieve the requisite level of transformation to secure sustainable contracts and Gursahaney, 2014). APA 66 What Is Clinic data fully accessible and of care. Clinical integr and healthcare Healthcare In healthcare val population, re care. In a clit clinical and care and adh to payers' in 4. Expand the POA care management structure. migraine and hypertension patients. Incentives berter-quali efficient us hospitals, care provi 9. Optimize deployment of staff. Policy Environment of Health Services Delivery Following vigorous and sometime contentious discussion, the PON board agreed to the following broadly stated goals for 2017-2019 1. Increase provider network participation 2. Design and expand the PQA information technology platform to 3. Develop full transparency and integration of data on the 5. Achieve better management of high-risk patients, 6. Establish clinical practice guidelines and related metrics for headachel 7. Connect PQA patients to nonclinical community resources. 8. Improve engagement of patients and caregivers in care planning, 10. Establish additional payer contracts based on value and shared savings opportunities, including preparing an application for the Medicare 8. You have been assigned by the PQA board to analyze the network's readiness to participate in Centers for Medicare & Medicaid Services sponsored accountable care organization programs. What criteria ca 2017-2019 goals? and proce providers bused car guideline Cli populat Shared Savings Program. chronic CASE STUDY QUESTIONS case m dition withir data healt ers, inad vide inte 1. Briefly explain the forces that led Pineridge Medical Center to launch PQA 2. List and evaluate the structures and tools PQA employs to improve patient quality and increase provider accountability. 3. What evidence shows that PQA follows best practices? 4. Explain why more hospitals in southeast Idaho have not joined PQA 5. How would you recruit more hospitals and clinicians in southeast Idaho, and how would you market PQA to them and other stakeholders 6. Develop a timeline showing PQA's key accomplishments. 7. How would you prioritize and operationalize PQA's proposed tion col w 1 be used to determine its readiness? HAD509 Written Case Analysis Content and Format (Adapted from: Simendinger, E. (2003). In Search of a Course Design and Teaching Methods to Improve Critical Thinking. Journal of Health Administration Education, 20(3), 197-213.) Do each case analysis without discussing it with other HAD 509 students prior to the due date. For each case, write the following information and number it 1 though 8 and use section headings: 1. Your name 2. The case number, case title, and class date. 3. 4. A summary of the case. [1 paragraph) This will require you to read the case several times. Do not just copy sentences from the case. Instead, express in your own words the essence of the case. A list of what you think are the 10-15 most important facts/factors in the case [1-2 pages). I page The most important health administration problem/issue to be solved in the case. [1 sentence]. 1 page List other secondary problems in the case [1-2 pages). 5. 6. Your recommended solution for the case (a.-d. below). Make clear specific realistic recommendations. There must be a clear logical sequence to your thoughts and recommendations. [4- 5 pages) a. At least three possible realistic alternative solutions for the most important problem (stated above for 5). b. Criteria to evaluate possible alternative solutions. For example: acceptability to stakeholders, needed resources, legality, timing, cost-effectiveness, ability to implement, side effects, qualifications, statistical data, financial data, ethical considerations, fit with case facts, likelihood of actually solving the problem, etc. c. Evaluation of the possible alternative solutions (6a) using the criteria (6b). d. Your recommended solution for the problem, based on 6a, 6b, and 6c. Justify your recommendation. 7. Specific MHA tools, methods, techniques, principles, theories, models, etc. from MHA courses that you used for this case. List specific tools (e.g., cost-benefit analysis, market segmentation, etc.). Do not list general subjects (e.g., finance, leadership) [1-2 pages]. 8. Answer any case study questions that accompany the case. If a case question is answered by what you already wrote for 3-7 above, then just note which part of your case analysis provides the answer. Submit your written reports by 11:55 pm on the Sunday of each week. chew A Case Study in Clinical Integration Pineridge Quality Alliance is a study in clinical integration, accountable care organizations, and population health. The case study profiles the his- . AIDS chase Merck .Org rek's Pineridge Quality Alliance be com of and Population CASE HISTORY/BACKGROUND tory, challenges , and opportunities related to development of a clinically integrated network and the sponsoring organization's quest to become an accountable care organization and engage in population health. In June, 2012, Brent Priday arrived in Pocatello, Idaho, as the newly appointed CEO of the 187-bed Pineridge Medical Center (Pineridge), which had been established in 2002 following the consolidation of Pocatello's two regional hospitals. Priday had served previously as CEO of West Valley Medical Center in Harrisburg, Oregon, where his 120-bed hospital participated in a "coordinated care organizationla new state- sponsored healthcare delivery model that seeks to lower costs and improve quality for Oregon Medicaid patients. Priday is convinced that coordi- nated care organizations and their variants are the wave of the future, and that Pineridge had to get onboard. 53 Policy Environment of Health Services Delivery Care Act in 2010 (U.S. Department of Health and Human Services, 2015) Priday believes that passage of the Patient Protection and Nicole healthcare business model, including reimbursement reductions, provides transforming the traditional from a Curve I (volume-based) to Curve 2 (value-based) paradigan (unes recapitalization and reconfiguration, and new payment models Though the pace of change will vary by market, Priday believes the readiness. The question looming for Priday and the Pineridge board is shift from Curve I to Curve 2 will happen irrespective of an organization's Wait and see: Maximize fee-for-service opportunities until the market 54 is a catalyst for disruptive forces that are & Gursahaney, 2014), Which of three common approaches should Pineridge take? . requires a shift or creates sufficient financial upside to do so. Be an early adopter. Create first-mover advantage by creating an accountable care organization/clinically integrated network to offset the impact of reduced reimbursement and utilization by increas ing market share of covered lives and keeping more of the services delivered to those living within our network. Hedge our bets: Experiment with pay-for-performance contracts and manage our health system's employee populations until more drastic change is warranted (Butts & Gursahaney, 2014). Since passage of the Affordable Care Act, over 750 accountable care organi- zations have been formed nationwide.? In advancing the concept of account- able care and the merits of clinical integration, Priday explained to Pineridge Medical Center's board of trustees that accountable care organizations are basically groups of doctors, hospitals, and other healthcare providers who organize voluntarily to give coordinated, high-quality care to Medicare and other patients. Coordinated care helps ensure that patients, especially the chronically ill get the right care, in the right place, at the right time, with the goal of avoiding unnecessary duplication of services and preventing medical errors. Priday noted that when an accountable care organization succeeds in both delivering high-quality care and spending healthcare dollars more wisely, it will share the savings it achieves for the Medicare program (Center for Medicare and Medicaid Services: Accountable Care Organizations, 2016). Priday knows his organization is not ready to form an accountable care organization per se and participate in accountable care organization pro- grams with the Centers for Medicare & Medicaid Services. Nevertheless, he understands the different kinds and types of accountable care organizations and is preparing his organization for eventual participation. A sample of accountable care organization programs sponsored by the Centers for Medicare & Medicaid Services is outlined in Table 4.1. Table 4.1. Centers for Medicare & Media Servo Medicare ACO type Launched Description Pinerilge Quality Alliance 2012 Initial ACO med Protection and A Medicare Shared Savings Program IMSSP) Pioneer ACO Model 2012 2013 Advance Payment ACO Model Designed specify for experience offering con centered care and AO arrangements Mots advanced texible than MSSP. Provides advance up front payment to ACOS MSSP model Designed to provide support to organizations whose wity to where the three-port im would be improved with a tional access to capital, including rural and physician-owned organisations An ACO model of prepaid shared savings that builds on the experience with the Advance Payment Model For HCOs experienced with ACOs-designed to assume more risk and reward. First disease-specific ACO model designed by CMS for Medicare beneficiaries with ESRD. 2015 ACO Investment Model 2015 Next Generation ACO Model Comprehensive End-Stage Renal Disease (ESRD) 2016 Source: Centers for Medicare & Medical Services (2016). CLINICAL INTEGRATION: A PREREQUISITE TO ACCOUNTABLE CARE From his experience in Oregon, Priday understands that development of a clinically integrated network is an essential precursor to establishment of an accountable care organization in southeast Idaho. Within days of his arrival at Pineridge, Priday advocated the merits of clinical integration and a Pineridge- sponsored clinically integrated network. With assistance from trusted advis- ers he developed a white paper on clinical integration that he shared with interested parties and potential stakeholders. The three-part paper addressed the questions: What is clinical integration? Who should clinically integrate? and Why should you clinically integrate? (See Appendix A.) THE PINERIDGE QUALITY ALLIANCE Priday and the Pineridge board decided that "being an early adopter" and "hedging our bets" were prudent choices. Ultimately, the Pineridge Policy Environment of Health Service Delivery Oy Alliance (POAclinically integrated network the bing higher increased teen themen contracts were extended to clinicians initially in Bannock and the Concurrent with its launch in late summer 2013, initial counties (POA's primary service area) with the goal of extending invitation to hospitals and clinicians in seven adjacent counties over next 12-36 months (Appendix B). POA contract addressed the folle ing key provisions: the need for transparency: joint contracting with insurance plans compliance with PQA initiatives including adher. ence to clinical benchmarks, participation in PQA-sponsored training and agreements to track and share quality performance measures and programs, and adoption of efficient and high-quality clinical practice dren of the dishes and their lider 56 in August 2013. POA has the following mission To be there am deste Table 4.2 Pinerid Momber name Brock Bailey, MD Camila Winom, M Donald Davis, ME Al Gomez, Raymond Marri Mia Wesley M Brand Priday J Abram Luciana Mart POA and December 19, 2011) INSURA INITIAT other data In Januar Idaho Ir with BB: Idaho. opined many to off rience Table respo Boa Net Pa LEADERSHIP AND STRUCTURE In the months leading up to and immediately following initiation of the PQA, the alliance was led by an external consultant. In September 2014, Karlyn Norton was hired as PQA's first full-time executive director. In August 2015, PQA hired Dr. David Bryan as its first full-time medical director. Bryan noted, "Pineridge Quality Alliance is the first and only clinically integrated network in eastern Idaho. It was founded and is oper- ated by physicians in the interest of improving quality and controlling the cost of medical care using robust and accurate data. It is clearly the future of medical care." Since its inception, PQA has been a physician-led organization, with a 9-person board of directors, 6 of whom are physicians (Table 4.2). In December 2013, the PQA governance structure was formed (Table 4.3). By mid-2014 the foundational governance and operating structures for POA were established (Table 4.3 and Figure. 4.1). Norton is especially pleased with the July, 2015, hiring of two full-time "care managers who coordinate care for patients with high-risk or chronic conditions , or who simply need someone to help them navigate the complicated healthcare system. INSURANCE COMPANY/PAYER CONTRACTS Table 4.2. Pineridge Ouality Alliance IPOAI board of director Pineridge Quality Alliance 57 Specialty Family medicine Cardiology Pediatrie Family medicine Family medicine Orthopedice Pinnridge Medical Center Administration CEO Pineridge Medical Center Administration ICFO Pineridge Medical Center Foundation ICEOX Member name Brock Bailey, MD (Chairs Camila Wicom, MD Donald Davis, MD Alexis Gomez, MD Raymond Marriott MD Mis Wesley, MD Brent Priday Jake Abram Luciana Martinez INITIATIVES In January 2014, Blue Cross ConnectedCare? became an offering on the Idaho Insurance Exchange. Previously, PQA had formed a partnership with Blue Cross of Idaho to manage patients who reside in southeast Idaho. Concerning its partnership with Blue Cross of Idaho, Norton opined "this is an extremely important venture and hopefully, the first of many partnerships with payers that allow PQA providers the opportunity to offer their patients a more guided and personalized healthcare expe- rience. By referring patients to the highest quality PQA providers and Table 4.3. Pineridge Quality Alliance governance structure: board and committee responsibilities Board of Directors Overall program oversight and decision-making author ity; budget approval committee participation approval Network Participation Provider participation criteria: recruitment and over- Committee sight of provider participation agreements Payer and Finance Oversight of contract terms, payer opportunities. Committee employee benefit plan, and financial distributions Quality, Utilization, and Creation of HIT infrastructure, reporting needs, and Health Information implementation plan; development of clinical Technology (HIT) performance measures for provider disease groups Committee and provider participants; and establishing utiliza- tion management targets Practice Administrators Feedback and recommendations on program deci- Advisory Council and sions related to ambulatory and inpatient clinical Operations Committee operations to quarterly, or as needed. Note: The Pineridge Quality Alliance board and subcommittees of the board meet bimonthly In July 2016, Norton explained that drastic changes were being made further incentivize patients to receive their care within the PQA network. . Piner partners Blue Cros Care POA and of Director 2014 PMC EC thro Blue n. 2015 Jan 2015 Ro the opportunity to more actively participate in their patients' downstream se. Only then will the alliance begin to coordinate care better, reduce newry procedures, and improve overall health status of those they Pharmacy management providers Analytics support July 2015 Ipport Credentialing Care Human Pineridge Qual A point maintenance HMO, partici a PPO, 2. UMA administra services 3.A certain management Mually Alliance, table of organisation care enti Berlying them navigate their services, PQA enables primary pro PC NE Going forward, the added copay and deductibles to patients who opt out of PQA will be so significant that far fewer services will be sought outside the network. The shift in plan design will reinforce the importance of staying in the network and allowing PQA to manage care more effectively than could be done with traditional preferred provider organization plans. In early 2015 PQA extended its relationship with Blue Cross of Idaho to support True Blue Medicare Advantage members in southeast Idaho, thus enabling PQA to perform population health and care man- agement activities for these more resource-intensive, difficult-to-manage Medicare patients. In mid-2015 PQA contracted with Regence BlueShield of Idaho on that insurer's Total Cost of Care program in southeast Idaho. Another population managed by PQA was Pineridge employees and their depen- dents (effective January 2015). This arrangement required an expansion from a physician-only network to one that included providers across the administrator. Founded in 1983 as United Medical Resources, UMA provides administrative allied health specialties (Table 4.5). The PQA network growth by selected Pineridge Quality Alliance Pineridge Quality Alliance partnership Table 4.4 Population health contract initiatives Non Humana, Pacific Source, and Aetna have expressed interest in partnering with maintenance organization (HMO) and preferred provider organization (PPO) plans. Like MMO participants designate an in-network physician to be their primary care provider. But 59 Summary Commercial point of vice Blue Cross of Idaho Connected Population estimate 1.700 members Commercial third party admin trator Population state 2.300 members Medicare Advantage henkman tenance organization. Population estimate 900 members Commercial preferred provider organization. Population et mate: 700 members. Dute Jan. 2014 Care PMC Employee Health Plan through UMRO Jan 2015 Blue Cross of Idaho True Blue Jart, 2015 Regence Blue Shield of Idaho Total Cost of Care July 2015 Pineridge Quality Alliance WaPpo. patients may go outside of the provider network for healthcare services services for self-funded health insurance plans. . A third-party administrator (TPA) is an organization that processes insurance claims or certain aspects of employee benefit plans for a separate entity entire continuum of care, including allied and ancillary professionals/ providers (see Table 4.4), thus allowing the provider network to sup- port the employee health plan's third-party administrator (UMR (United Medical Resources]). Norton said the hospital is interested in using its new clinically integrated network to prove it could deliver better quality care for employees at lower overall cost. A summary of these population health-related contracting initiatives is provided in Table 4.4. NETWORK DEVELOPMENT AND GROWTH Two years following inception, PQA included 580 clinicians from 7 provider groups representing not-for-profit, for-profit, public, private, urban, and rural-based domains all working toward a common goal of clinical transformation and collaboration consistent with the Institute for Healthcare Improvement Triple Aim. By fall 2016, PQA included representation from over 30 medical and specialties is outlined in Table 4.6. Policy Environment of Health Services Delivery Table 45 Pineridge Quality Alliance network and specialty composition they don 60 Otorhinolaryngology Pediatrics Home het Hospice in a clinically the POA fee sch of PQA-insuran critical access hac POA: she unde will be limited grated network Anesthesia Ambulatory surgery center Behavioral health Physicalloccupational speech therapy Podiatry Psychiatry Psychology Independent lab Internal medicine Nephrology Neurology CLINICAL TOOLS-P Cardiology Chiropractic Durable medical equipment Endocrinology Family practice Gastroenterology Obstetrics bynecology Ophthalmology Optometry Pulmonology Radiology Skilled nursing facilityong term acute care unit Urgent care Urology Not surpris by early 20 clinically tice manag Orthopedics General surgery tools kno firm (Ad- Davis ex observir The PQA was relatively successful in recruiting participation from physicians and allied health professionals in Bannock County, but by early 2016 the alliance had been unable to secure contracts with surrounding critical access hospitals and clinicians in southeast Idaho (Appendix B, District 6). Norton explains that these rural, independent hospitals and their local physicians do not feel any urgency to change. She also believes have me exist, a collect Advan Table Hel and cie Table 4.6. Pineridge Quality Alliance network growth by selected specialties 2014 2015 2016 Provider types 185 213 240 Family practice 12 13 17 Internal medicine 8 9 9 Pediatrics 12 Obstetrics/gynecology 12 12 14 Orthopedics 16 16 Cardiology 16 25 25 General surgery 7 7 Behavioral health 33 Chiropractic Physical occupational/speech therapy 111 133 Home health/hospice 9 16 Other 408 492 45 5 135 16 527 in a clinically integrated network. Some base they don't fully understand the purpose of the POA fee schedule) to care for patients they were of POA-insurance company contracts, North POA: she understands that without a reader en PON will be limited in its ability to fully realize the nefits in critical acces hospitals in the regionsresowe grated network (see Appendix A. Why should yodinically Nor surprisingly, the more than 70 organizations that made up the POA tice management systems. To facilitate realization of the benefits of a truly by early 2014 employed many kinds and types of medical records and clinically integrated delivery system, in mid-2014 PQA purchased a set of firm (Advisory Board Company, 2016). PQA board member Dr. Donald rools known as Crimson from the Advisory Board Company, a consulting Davis explains that Crimson "will allow us to start collecting data and observing quality measures from all providers in the network. Once we have meaningful data we can decide where there is variation, why outliers exist, and how we can implement strategies to improve our individual and TOOLS-PROGRAMS-SERVICES collective outcomes. The three modules that make up Crimson Clinical Pineridge Quality Alliance CLINICAL INTEGRATION Advantage are outlined in Table 4.7. Table 4.7. Crimson Clinical Advantage Crimson Continuum of Care Helps hospitals achieve the physician alignment needed to advance quality goals and secure cost savings. Places credible performance profiles in the hands of physi- cians, enabling them to better meet healthcare organization cost and quality goals. Crimson Population Risk Management Helps hospitals manage total cost and quality for defined populations including self-insured employee plans-and inform risk-based contract negotiations with payers. Combines insight on health system strategy with a robust benchmarking database and clinical algorithms; physicians get a 360-degree view of patient care, including an evaluation of the organization's strengths and liabilities, and more. Crimson Care Management Helps hospitals create and run effective, collaborative care management programs by providing intelligent workflows and integrating complex data sources to custom- ize care programs and drive compliance. Generates data that will unlock actionable insights that help care managers work smarter and maximize impact. network with access to powerful data is that we start to pay attention to our patients overall health, no matter where they receive the together as a collective team to provide the highest quality care, WW care, because we now have visible data. And, because we are now working the entire network of PQA providers to do well, not just ourselves Concerning Crimson Care Management, Norton notes that Crim reams. Crimson generates to-do tasks, alerts, and reminders in response to analyzes data fast enough to provide real-time updates to patient care patient admission, discharge, or care program data. It then routes action as needed. The Crimson Population Risk Management tool can easily requests to the appropriate care team members for prompt intervention, track member, population, and provider progress toward organizational clinically integrated Davis explains that one important benefit to a truck bor Additions to practic problems provided CLINI In con Policy Environment of Health Services Delivery and contractual goals. In elaborating the merits of clinical integration and the need for population health and care management, Norton often uses Figure 4.2 as an example of how the Crimson software categorizes populations into high-risk, rising-risk, and low-risk care categories. Once the population is risk stratified, providers can focus on persons who need the most help. Norton further explains that Crimson software integrates data from patient registries, electronic health records, and other practice management systems to improve coordination of care delivery between and among primary and special practices and hospitals. Since 2014, PQA has implemented the capabilities of Crimson Continuum of Care at each physician site, enabling these providers to provid perfos tinec Systet and to be exp Qu (Ar +8 E Meet Your Three Patient Populations HIGH PATIENT COMPLEXITY DRIVING OUTSIZED PATIENT COSTS... ..REQUIRES CREATING THREE UNIQUE PATIENT POPULATIONS WITH THREE COMPLEMENTARY CARE MODELS PERCENTAGE OF MEDICARE BENEFICIARIES HIGH-RISK SW OF POPULATION PERCENTAGE OF TOTAL MEDICARE SPENDING RISING RISK 20% OF POPULATION LOW RISK 754 OF POPULATION MM OF CONCTIONS HOORONE ho ME SOKOR MORE Figure 4.2. Crimson Capabilities (Advisory Board Company, 2016). track both aggregate and patient-specific clinical and final data Additionally, POA staff provides agregate and peactice-pecific reports problems represent opportunities for improvement. Sample reports to practices and selected PQA committees. Provider and patient-specific CLINICAL AND OPERATIONAL MEASURES In conformance with the POA Participating Provider Ngreement, POA performance improvement and data-sharing initiatives to share data con providers agree to actively and meaningfully participate in the alliance's trined in medical records, billing, claims, practice management, or other systems, clectronic, or otherwise. In fall 2014, the PQA Quality, Utilization, Pineridge Quality Alliance in and HIT committee, with approval of the PQA board, selected 15 measures to begin tracking and analyzing. Donald Davis, a pediatrician on the board, explains "These are Physician Quality Reporting System and National (Appendix D). In 2015, PQA legal counsel recommended the alliance add 48 more measures: 5-10 per major provider type for a total of 63 measures. EDUCATION AND TRAINING In November 2014, PQA leaders announced it would collaborate with Optum" to provide a series of educational opportunities focused on the Medicare Advantage Risk Adjusted Program and the Medicare Access and CHIP Reauthorization Act of 2015. Norton reported the following: Optum works with healthcare professionals and health plans to help them attain improved health outcomes. With relevant tools and support, Optum can help healthcare providers in the early detection, ongoing assessment, and accurate reporting of chronic conditions. ... Optum has technology and health intelligence solutions that help providers accu- rately document and code conditions while improving the overall quality of care.... The investment in technology, education, and training is key to PQA's ability to achieve the noted "Triple Aim." Buck Ridley, PQA's information technology specialist, observed in the first year (following implementation of the Crimson and Optum initia- tives) "we will be able to see, individually and collectively as an alliance, where the opportunities for improvement are. By year 5, we will use the information in a sophisticated manner to improve the overall cost, quality, and utilization of care we deliver." community to improve quality and reduce costs of care for their emplo ces. Additional quality measures, clinical pathways, and care management At the June 2016, PQA board retreat Priday addressed the following . Succeeding in population health requires more than completing a either due to their insufficient payer capabilities or limited geographic 6-4 POA works in o rurality, We don't h have. Thu our comm allow our need with Policy Environment of Health Seri Delivery LOOKING BACK LOOKING AHEAD Reminiscing three years following is inexp. PCROP observed. We wanted to create profil hanged patient care that will directly affect the health of time in which our industry has been turned on its head rem it limits, we have intimated transformation that will repite even mere from us than has already been dered Three years following is loch, POA has invested renghly $2.5 million administrators and clinicians have invested well in excess of 2016 in planning and implementation related activities. The future include ships, working with Human regarding opportunities for their Medicar Advantage members, partnering with Aetna on their commercial The ger our pro and que consun differs that we Alth thes cian thes sti th Inf pli ne pe . programs represent other opportunities for developing improvement challenges common to the industry: Medicare Shared Savings Program application and creating a Federal Trade Commission-compliant structure. Creating an effective and scalable population health/clinical integra- tion infrastructure requires a significant investment of capital, time and resources. It is extremely difficult to align providers across the care continuum in a way that drives quality and sufficient cost savings to create meaningful shared savings dollars. The financial benefits of shared savings programs are directed at poi mary care physicians and are inherently short term unless they incor porate bundled payments as a means to engage specialists and focus on reducing spending on high-cost procedures. Payers are often unwilling to structure mutually beneficial contracts with networks that offer sufficient upside potential to offset losse in fee-for-service revenue because the networks have unproven track records or lack sufficient geographic reach to meet access requirements. Not all networks are capable of contracting directly with employers coverage for a broad employee base. challenges specific to POA: In the context of these industry-wide ises, Norton disco POA has unique challenges compared with dinically integrated works in other parts of the county due to i topography We don't have the span of providers and specialties that makes our community to form lasting and collaborative partnerships that will have. Thus it's critical for us to all with independent power allow our patient populations to access the high-value services they The geographic, rural, and relatively sparsely populated nature of our provider community means we must strive for excellence in con and quality and to have an accurate measure of what the healthcare consumer perceives as "value" because their definition may be quite different from ours. As consumers become more savvy. we must ensure that what we offer meets their expectations. . Although PQA board members publicly affirm their commitment to their practices is difficult. One prominent board member privately successfully navigate the transition from Curve I to Curve 2" (Butts & Pineridge Quality Alliance rurality leaving . . the clinically integrated network, getting those leaders and other physi- stated, "Honestly, I'm not sure I get it. Crimson is complex and I'm still not using the data to change or improve my practice." Even though the PQA medical director is talented and committed to the cause, he is stretched too thin and unable to meet with network physicians and clinicians to teach, motivate, or monitor their performance, In frustration, Norton occasionally reaches out to a seasoned and accom- plished mentor from across the state. "Look" the mentor said, your network is new and small, but look at what you have accomplished...be patient, learn to fail 'as fast and inexpensively as possible'... and just keep moving forward!" Priday and Norton say their observations/conclusions should not lead PQA to abandon its clinically integrated network and eventual account- able care organization strategy because pressure from employers to reduce premiums and the government's expansion of value-based programs will continue, regardless. Rather, they contend, "If we are going to be paid differently, we must organize and deliver care in a way that leads to dif- ferent results. Developing our clinically integrated network is a way f