

Question: In January, Mark Amsted, M.D., Chair of Obstetrics and Gynecology at Brookstone Medical School, Chief of Ob-Gyn at Brookstone Medical Center, and President of Brookstone
In January, Mark Amsted, M.D., Chair of Obstetrics and Gynecology at Brookstone Medical
School, Chief of Ob-Gyn at Brookstone Medical Center, and President of Brookstone Ob-Gyn
Associates (BOGA), was preparing to meet with the Harris National Bank. He planned to present a
request for a $300,000 line of credit, the approval of which was critical to BOGAs continued operations. He had discussed the need for the line of credit with the Dean of the Medical School, and
had obtained approval to make the request to the bank, but he was by no means certain that the bank
would agree to the loan. A great deal depended upon the banks reaction to the financial information that he and his business manager, Randy Weber, planned to present.
BACKGROUND
BOGA was a faculty practice plan comprised of university faculty physicians in obstetrics and
gynecology (Ob-Gyn). All BOGA physicians were on the staff of Brookstone Medical Center
(BMC), one of the citys major teaching hospitals. The hospital was affiliated with the Brookstone
Medical School, and all of BOGAs physicians held faculty appointments in the medical school.
BOGA had been organized several years earlier as a nonprofit educational trust. Initially, its
offices had been located in the hospital, and it had grown slowly. During its first few years of existence, BOGAs physicians saw mainly Medicaid, Medicare, and self-pay (or uninsured) patients in
the hospitals outpatient department.
Several years ago, Brookstone Medical Center began to experience declining Ob-Gyn admissions due to competition from some nearby community hospitals. As a result, BMC offered to contribute $1 million to BOGA if it would open offices in a nearby building. The idea was to make
BOGAs facilities more attractive to patients with private insurance, in the hope that these patients
would use its services. If the idea worked, BMC would reverse the declining trend in its Ob-Gyn
admissions, and would do so with fully insured patients. After discussing BMCs proposal with
his colleagues, Dr. Amsted accepted the offer.
Dr. Amsted supplemented the $1 million contribution from the medical center with a long-term
note from the Harris National Bank. The funds were used to purchase new medical and office
equipment, renovate the space, and furnish the offices in the new facility.
The surrounding community responded positively to BOGAs move. The reputation of
BOGAs physicians and the attractiveness of the new facilities led to increases in the number of
private insurance patients treated. In each of the last two years, BOGAs revenue had increased by
about 20 percent over the previous year.
PROBLEMS
Despite the growth in revenues, BOGAs profitability was becoming an issue. Indeed, as he
began to prepare for his meeting with the bank, Dr. Amsted was quite perplexed. He commented:
Its crazy. Despite our rapid rate of growth, were losing money, and I dont understand why. Our salaries are
competitive and our physicians see as many patients per hour as Ob-Gyn physicians in other places. Our
scheduling is good, so we dont have a lot of downtime. All our other costs seem quite reasonable. Yet, the
figures speak for themselves. Last year, we lost $850,000!
According to Randy, if we dont get the line of credit from the bank, we wont be able to meet some of
our payroll and other expenses next month. Even if the bank gives us the loan, Im sure theyll ask me to
either cut expenses or increase our charges so well be profitable. The problem is that the charges are restricted by our third parties, and I can see no place to cut expenses other than by laying people off. Im reluctant to do that, though, since everyone seems overworked.
MODIFIED CASH ACCOUNTING
BOGA used what was called a modified cash form of accounting. Under this system, with only
one exception, revenue is recorded when cash is received, and expenses are reported when cash is
paid out. The exception is equipment and other fixed assets, where the cash payment associated
with a purchase is not treated as an expense. Rather, because each asset has a relatively long service
life (usually five to ten years for equipment), an annual depreciation figure is computed by dividing
the cost of the equipment by its estimated service life. This depreciation figure is shown as an expense on the operating statement even though it is not represented by an actual cash payment (the
cash payment is made when the equipment is purchased).
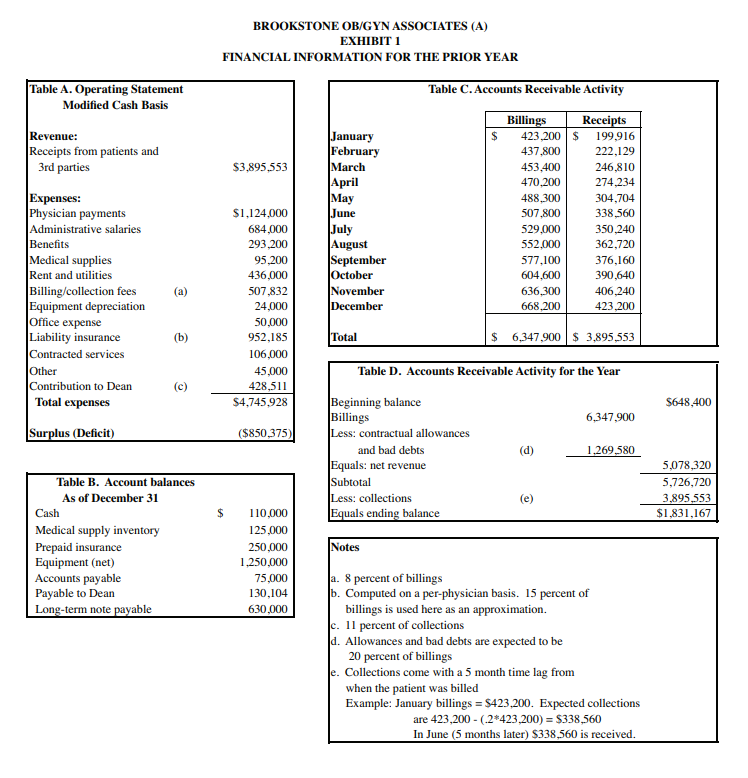
Exhibit 1 contains financial information for BOGAs operations during the prior year. As it
shows (Table C), although BOGA billed patients for $6.3 million, it received only $3.9 million in
cash during the year. The difference, less Mr. Webers estimate of $1.3 million of contractual allowances and bad debts on the $6.3 million, went into its accounts receivable. Accounts receivable
grew from $648,400 at the beginning of the year to $1.8 million as of the end of the year (Table
D). Exhibit 1 also shows BOGAs operating statement for the year (Table A). With revenue of
$3.9 million and expenses of $4.7 million, BOGAs operating deficit slightly exceeded $850,000
for the year.
ACCRUAL ACCOUNTING
Alice Tanshel, the Harris Banks lending officer, had asked Dr. Amsted to come to the meeting
with financial statements prepared on both a modified cash and an accrual basis. In accrual accounting, revenue is recognized when it is earned (usually when the bill is sent out) rather than
when the cash is collected. Similarly, expenses are recorded when they are incurred, rather than
when the associated cash is paid out.
The main difference between the two approaches for BOGA was in the amount of revenue. The
switch to an accrual basis would require Mr. Weber and BOGAs accountants to record revenue
when services were delivered to a patient, rather than when cash was received. Because of this, Mr.
Weber needed to estimate the portion of revenue that would not be collected. Contractual allowances by third party payers, as well as the fact that some patients would never pay their bills, meant
that not all revenue that was billed actually would be collected. This was not a problem with the
modified cash basis, since cash payments and revenue were the same. However, the switch to an accrual basis required Mr. Weber to make estimates of the allowances and bad debts. Net revenue
was the difference between billings and these estimates.
Mr. Weber commented on the task that lay before him:
I remember learning about accrual accounting in school. Even then, it wasnt clear to me why its advantageous to use it. With the modified cash system, life is quite simple. When we get a check, weve earned
revenue. We dont have to worry about estimating bad debts formally, we just need to know about how
much we can expect to collect. When we pay out cash, except for equipment, we have an expense. What
could be easier to understand?
Preparing a set of accrual statements is going to be a nightmare. Ive spoken with our accountants, and
they tell me that to prepare the statements for the bank, Im going to have to estimate more than just revenues. Inventory, for example. Under the modified cash system, when we buy some medical supplies, we
have an immediate expense. With the accrual system, we need to create an inventory, and we only incur an
expense when we use an item, rather than when we buy it. Insurance is just like inventory. With an accrual
system, we record the expense when we use the insurance, not when we pay the premium to the insurance
company. Thats a bit of a complication since we pay our premiums for several months in advance; it leads
to what the accountants call a Prepaid Insurance account.
Accounts payable is just the opposite. Our vendors let us charge our supply purchases, and under the
modified cash system we incur an expense when we pay a vendor. Not with the accrual system. But this is
really tricky. When we buy some medical supplies, the goods go into inventory, and, as I said, we incur an
expense when we use the inventory. But this means we can incur an expense even if we havent paid the
vendor yet. This is not just complex; its layers of complexity!
Finally, the accountants tell me that after we deduct our estimates of allowances and bad debts from
billings, we owe the Dean 11 percent of this net revenue, as they call it. Although the Dean doesnt ask
us to pay him until we receive the cash, the accountants tell me we need to keep track of the difference. Let
me give you an example. Last year, our net revenue was $5,078,320 [see Table D of Exhibit 1]. At the
11% rate, we owed the Dean $558,615. By contrast, on a modified cash basis, we owed (and paid) the Dean
TCG161 Brookstone Ob-Gyn associates (A) 2 of 5
$428,511, or 11 % of our $3,895,553 in cash receipts [see Table A in Exhibit 1]. Thats a difference of
$130,104. The accountants tell me that this amount is a liabilitywe owe it to the Dean. Even though we
dont have to pay him until we collect the cash, we still have to show the liability on our balance sheet
 1. Using an accrual system, prepare an operating statement for the year and a balance sheet as of December 31. What do these statements tell you about BOGAs profitability?
1. Using an accrual system, prepare an operating statement for the year and a balance sheet as of December 31. What do these statements tell you about BOGAs profitability?
2. In the absence of the banks stipulation that accrual be used, which type of systemmodified cash or accrualwould you recommend that Dr. Amsted use for BOGA? Why?
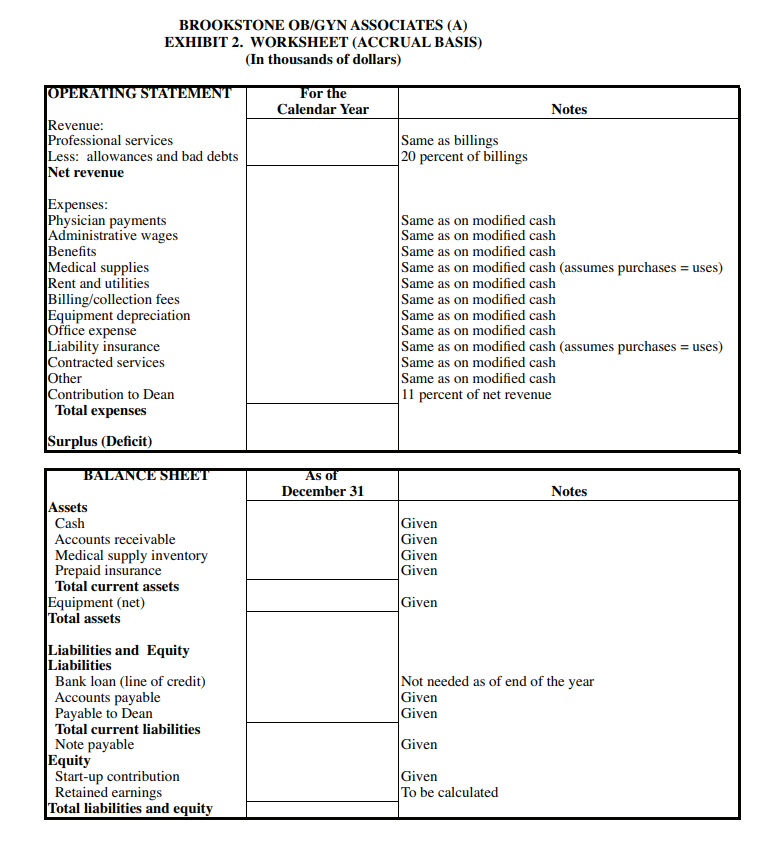
PREPARING FOR THE MEETING To prepare for the meeting with the bank, Dr. Amsted asked Mr. Weber to construct both an operating statement and a balance sheet using the accrual method. The operating statement would be for the entire calendar year, whereas the balance sheet would be as of December 31. The accountants had provided Mr. Weber with a worksheet (Exhibit 2) to use in preparing the two statements. They also had given him their assessment of some of the account balances as of December 31. These are shown in Table B of Exhibit 1. With this information in hand, Mr. Weber began to prepare a set of financial statements on an accrual basis. Assignment 1. Using an accrual system, prepare an operating statement for the year and a balance sheet as of December 31. What do these statements tell you about BOGA's profitability? 2. In the absence of the bank's stipulation that accrual be used, which type of system-modified cash or accrual - would you recommend that Dr. Amsted use for BOGA? Why? BROOKSTONE OB/GYN ASSOCIATES (A) EXHIBIT 1 FINANCIAL INFORMATION FOR THE PRIOR YEAR Table C. Accounts Receivable Activity Table A. Operating Statement Modified Cash Basis Revenue: Receipts from patients and 3rd parties $3,895,553 Expenses: Physician payments Administrative salaries Benefits Medical supplies Rent and utilities Billing/collection fees Equipment depreciation Office expense Liability insurance Contracted services Other Contribution to Dean Total expenses January February March April May June July August September October November December $1,124,000 684,000 293,200 95,200 436,000 507,832 24,000 50,000 952,185 106,000 45,000 428,511 $4,745.928 (a) Billings Receipts 423,200 $ 199,916 437,800 222.129 453,400 246,810 470,200 274,234 488,300 304,704 507.800 338,560 529.000 350.240 552.000 362,720 577,100 376,160 604.600 390.640 636,300 406,240 668,200 423,200 (b) Total $ 6,347,900 $ 3.895,553 (c) $648,400 Surplus (Deficit) ($850,375) Table D. Accounts Receivable Activity for the Year Beginning balance Billings 6,347.900 Less: contractual allowances and bad debts (d) 1.269,580 Equals: net revenue Subtotal Less: collections (e) Equals ending balance 5,078,320 5,726,720 3,895,553 $1,831,167 $ Table B. Account balances As of December 31 Cash Medical supply inventory Prepaid insurance Equipment (net) Accounts payable Payable to Dean Long-term note payable Notes 110,000 125,000 250,000 1,250,000 75.000 130,104 630,000 a. 8 percent of billings b. Computed on a per-physician basis. 15 percent of billings is used here as an approximation. c. 11 percent of collections d. Allowances and bad debts are expected to be 20 percent of billings le. Collections come with a 5 month time lag from when the patient was billed Example: January billings = $423,200. Expected collections are 423,200 - (-2*423,200) = $338,560 In June (5 months later) S338,560 is received. BROOKSTONE OB/ GYN ASSOCIATES (A) EXHIBIT 2. WORKSHEET (ACCRUAL BASIS) (In thousands of dollars) OPERATING STATEMENT For the Calendar Year Notes Revenue: Professional services Same as billings Less: allowances and bad debts 20 percent of billings Net revenue Expenses: Physician payments Same as on modified cash Administrative wages Same as on modified cash Benefits Same as on modified cash Medical supplies Same as on modified cash (assumes purchases = uses) Rent and utilities Same as on modified cash Billing/collection fees Same as on modified cash Equipment depreciation Same as on modified cash Office expense Same as on modified cash Liability insurance Same as on modified cash (assumes purchases = uses) Contracted services Same as on modified cash Other Same as on modified cash Contribution to Dean 11 percent of net revenue Total expenses Surplus (Deficit) BALANCE SHEET As Of December 31 Notes Assets Cash Accounts receivable Medical supply inventory Prepaid insurance Total current assets Equipment (net) Total assets Given Given Given Given Given Not needed as of end of the year Given Given Liabilities and Equity Liabilities Bank loan (line of credit) Accounts payable Payable to Dean Total current liabilities Note payable Equity Start-up contribution Retained earnings Total liabilities and equity Given Given To be calculated PREPARING FOR THE MEETING To prepare for the meeting with the bank, Dr. Amsted asked Mr. Weber to construct both an operating statement and a balance sheet using the accrual method. The operating statement would be for the entire calendar year, whereas the balance sheet would be as of December 31. The accountants had provided Mr. Weber with a worksheet (Exhibit 2) to use in preparing the two statements. They also had given him their assessment of some of the account balances as of December 31. These are shown in Table B of Exhibit 1. With this information in hand, Mr. Weber began to prepare a set of financial statements on an accrual basis. Assignment 1. Using an accrual system, prepare an operating statement for the year and a balance sheet as of December 31. What do these statements tell you about BOGA's profitability? 2. In the absence of the bank's stipulation that accrual be used, which type of system-modified cash or accrual - would you recommend that Dr. Amsted use for BOGA? Why? BROOKSTONE OB/GYN ASSOCIATES (A) EXHIBIT 1 FINANCIAL INFORMATION FOR THE PRIOR YEAR Table C. Accounts Receivable Activity Table A. Operating Statement Modified Cash Basis Revenue: Receipts from patients and 3rd parties $3,895,553 Expenses: Physician payments Administrative salaries Benefits Medical supplies Rent and utilities Billing/collection fees Equipment depreciation Office expense Liability insurance Contracted services Other Contribution to Dean Total expenses January February March April May June July August September October November December $1,124,000 684,000 293,200 95,200 436,000 507,832 24,000 50,000 952,185 106,000 45,000 428,511 $4,745.928 (a) Billings Receipts 423,200 $ 199,916 437,800 222.129 453,400 246,810 470,200 274,234 488,300 304,704 507.800 338,560 529.000 350.240 552.000 362,720 577,100 376,160 604.600 390.640 636,300 406,240 668,200 423,200 (b) Total $ 6,347,900 $ 3.895,553 (c) $648,400 Surplus (Deficit) ($850,375) Table D. Accounts Receivable Activity for the Year Beginning balance Billings 6,347.900 Less: contractual allowances and bad debts (d) 1.269,580 Equals: net revenue Subtotal Less: collections (e) Equals ending balance 5,078,320 5,726,720 3,895,553 $1,831,167 $ Table B. Account balances As of December 31 Cash Medical supply inventory Prepaid insurance Equipment (net) Accounts payable Payable to Dean Long-term note payable Notes 110,000 125,000 250,000 1,250,000 75.000 130,104 630,000 a. 8 percent of billings b. Computed on a per-physician basis. 15 percent of billings is used here as an approximation. c. 11 percent of collections d. Allowances and bad debts are expected to be 20 percent of billings le. Collections come with a 5 month time lag from when the patient was billed Example: January billings = $423,200. Expected collections are 423,200 - (-2*423,200) = $338,560 In June (5 months later) S338,560 is received. BROOKSTONE OB/ GYN ASSOCIATES (A) EXHIBIT 2. WORKSHEET (ACCRUAL BASIS) (In thousands of dollars) OPERATING STATEMENT For the Calendar Year Notes Revenue: Professional services Same as billings Less: allowances and bad debts 20 percent of billings Net revenue Expenses: Physician payments Same as on modified cash Administrative wages Same as on modified cash Benefits Same as on modified cash Medical supplies Same as on modified cash (assumes purchases = uses) Rent and utilities Same as on modified cash Billing/collection fees Same as on modified cash Equipment depreciation Same as on modified cash Office expense Same as on modified cash Liability insurance Same as on modified cash (assumes purchases = uses) Contracted services Same as on modified cash Other Same as on modified cash Contribution to Dean 11 percent of net revenue Total expenses Surplus (Deficit) BALANCE SHEET As Of December 31 Notes Assets Cash Accounts receivable Medical supply inventory Prepaid insurance Total current assets Equipment (net) Total assets Given Given Given Given Given Not needed as of end of the year Given Given Liabilities and Equity Liabilities Bank loan (line of credit) Accounts payable Payable to Dean Total current liabilities Note payable Equity Start-up contribution Retained earnings Total liabilities and equity Given Given To be calculated
Step by Step Solution
There are 3 Steps involved in it

Get step-by-step solutions from verified subject matter experts