Question: 1-4 please not to wordy Chapter Cases Case Studies Read St. John's Reengineering in the Case Studies section at the end of this book. What
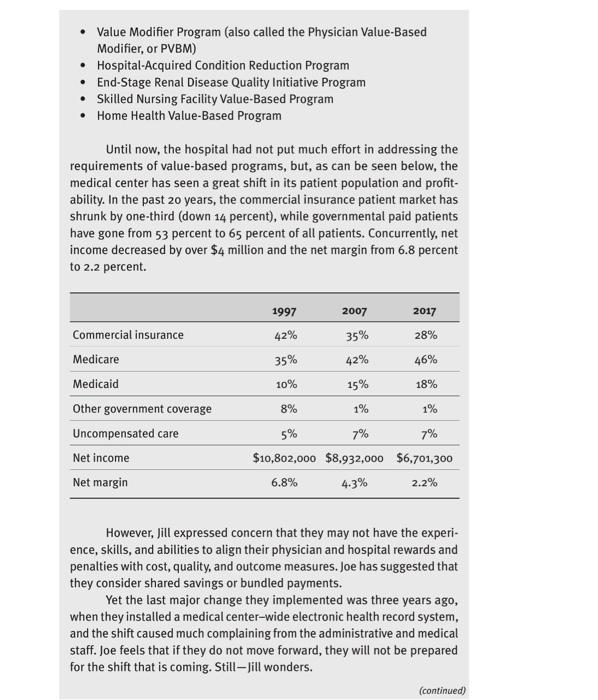
Chapter Cases Case Studies Read "St. John's Reengineering" in the Case Studies section at the end of this book. What did the administration of this organization do wrong during the implementation of its strategic changes? Read "Dissolving a Long-Standing Affiliation and Moving On" in the Case Studies section at the end of the book. Review and discuss the ques- tions at the end of the case. A Shift to a "Value-Based Care" Organization Jill, the CEO of Redmond Medical Center, and her assistant, Joe, attended the American College of Healthcare Executives (ACHE) annual Congress last week and, upon comparing notes, they concurred that moving healthcare to "value-based care" appeared to be the direction of most of the country's providers. As defined at the ACHE meeting, value-based care models focus on the value received by patients by rewarding better outcomes, which moves a health provider away from the traditional fee-for-service model that rewards for more volume. Few systems have moved away from the volume, fee-for-service model to a value-based system. In 2016, only 27 percent of healthcare provider organizations had experimented with or completed value-based pilot pro- grams (Sanicola 2017). However, employers, health insurance companies, and government purchasers have begun to encourage providers to transition to value-based payment models. For example, the Centers for Medicare & Medicaid Services (CMS) had implemented value-based programs primarily for Medicare patients with the goal to link provider performance of quality measures to provider payment. These included the following: Hospital Value-Based Purchasing Program Hospital Readmission Reduction Program Value Modifier Program (also called the Physician Value-Based Modifier, or PVBM) Hospital-Acquired Condition Reduction Program End-Stage Renal Disease Quality Initiative Program Skilled Nursing Facility Value-Based Program Home Health Value-Based Program Until now, the hospital had not put much effort in addressing the requirements of value-based programs, but, as can be seen below, the medical center has seen a great shift in its patient population and profit- ability. In the past 20 years, the commercial insurance patient market has shrunk by one-third (down 14 percent), while governmental paid patients have gone from 53 percent to 65 percent of all patients. Concurrently, net income decreased by over $4 million and the net margin from 6.8 percent to 2.2 percent. 1997 2007 2017 Commercial insurance 42% 35% 28% Medicare 35% 42% 46% Medicaid 10% 15% 18% Other government coverage 8% 1% 1% Uncompensated care 5% 7% 7% Net income $10,802,000 $8,932,000 $6,701,300 Net margin 6.8% 4.3% 2.2% However, Jill expressed concern that they may not have the experi- ence, skills, and abilities to align their physician and hospital rewards and penalties with cost, quality, and outcome measures. Joe has suggested that they consider shared savings or bundled payments. Yet the last major change they implemented was three years ago, when they installed a medical center-wide electronic health record system, and the shift caused much complaining from the administrative and medical staff. Joe feels that if they do not move forward, they will not be prepared for the shift that is coming. Still - Jill wonders. (continued) Questions 1. What could fill and Joe do to understand their level of preparedness for change more fully? 2. Who would be the key stakeholders for the proposed changes? 3. Why should Jill and Joe expect resistance to this type of change and what could they do to address it? 4. What should they do before they decide to go ahead with this change