

Question: A doctor has come to you to develop a database to help track the results of a vaccine trial. You will receive information from the
A doctor has come to you to develop a database to help track the results of a vaccine trial. You will receive information from the doctor that will include an organizational document, some policies and procedures for the testing, and you will be able to speak with the doctor himself to answer any questions. The doctor doesnt want anything super complex. He just wants to be able to track the patients in the trial, the clinicians involved with the trial, and the results of the trial at each visit.
Based on the business rules that you discover from the information given, create an Entity-Relationship diagram for the database the doctor requires. Create the entity-relationship diagram using crows foot notation.
Below are the files and rules given to help create the ERD.
After speaking with the doctor and the administrator, you have determined the following additional information as business rules:
1. The organization holding the trial has three types of EMPLOYEES: Doctors, Nurses, and Staff. Doctors and Nurses are special cases of employees. Doctors have a DEA license number and DEA license number expiration date. Nurses have a nursing certificate number and whether they are an RN or a BSN.
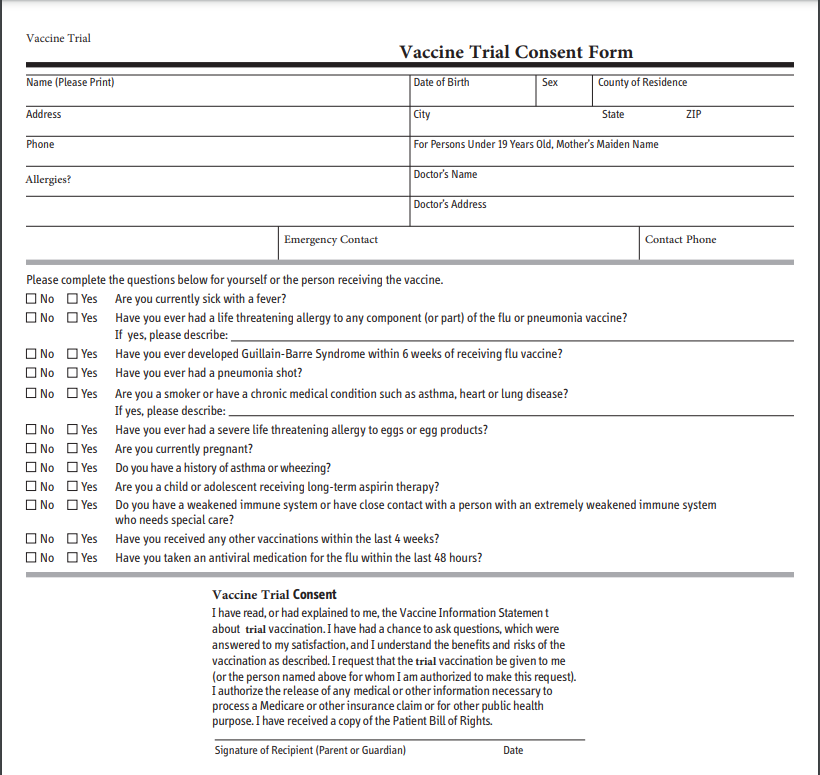
2. On the PATIENT form, any yes answer disqualifies the patient from the trial, so for the sake of the DB, you do not have to put fields for each of the qualifying questions, but rather just one field indicating whether they are qualified.
3. PATIENTS are divided into two different types, trial and placebo. These types carry no attributes that are specific to them.
4. PATIENTS do not to have an ALLERGY, but they could have many allergies.
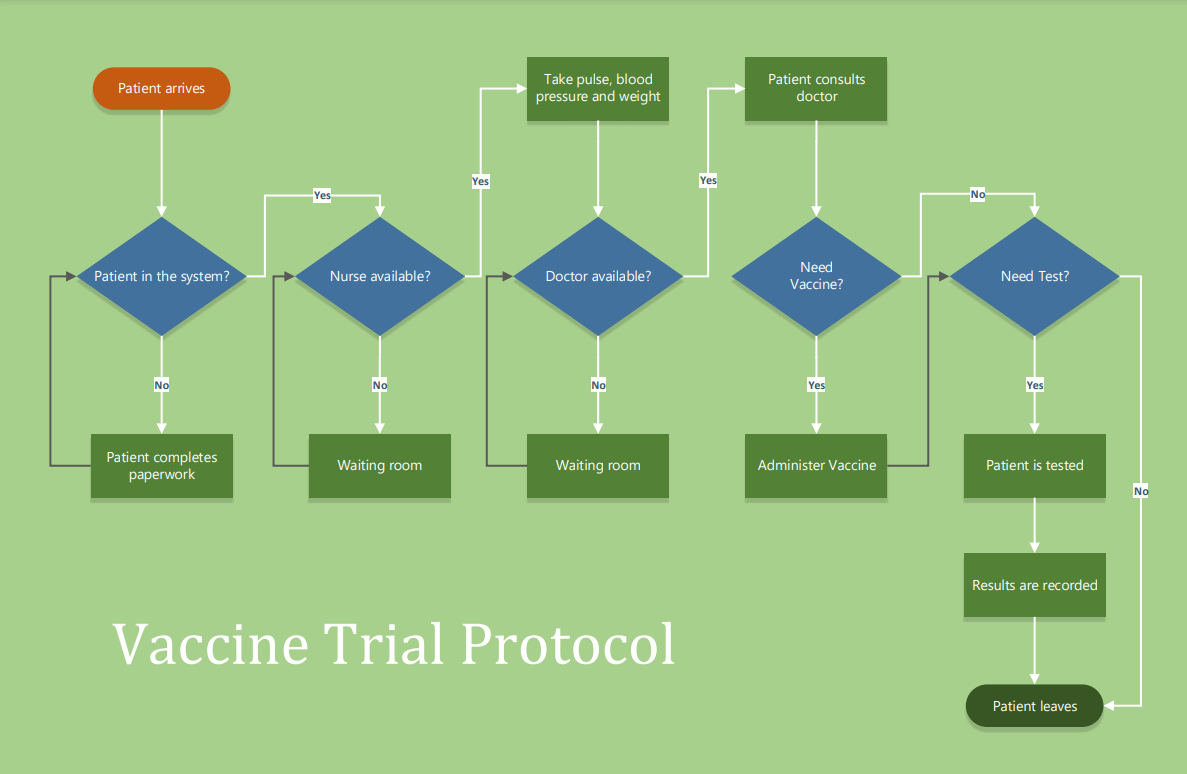
5. On a VISIT their vital signs are taken as shown on the flowchart, they are then administered the vaccine and the information from the bottom of the consent form is filled out. The time and date of the visit as well as the Doctor and Nurse that saw the patient are recorded as well as the results of the test for effectiveness.
6. A PATIENT does not have to go for a VISIT (they can opt-out), but a VISIT is made by only one PATIENT at a time.
7. A VISIT must have a Doctor and a Nurse. There are only one Doctor and Nurse on each VISIT, but they can be a part of many different VISITS.
8. This trial only has one administration of the vaccine.
Patient arrives Take pulse, blood pressure and weight Patient consults doctor Yes Yes Yes No Patient in the system? Nurse available? Doctor available? Need Vaccine? Need Test? No No No Yes Yes Patient completes paperwork Waiting room Waiting room Administer Vaccine Patient is tested No Results are recorded Vaccine Trial Protocol Patient leaves Vaccine Trial Vaccine Trial Consent Form Date of Birth County of Residence Name (Please Print) Sex Address City State ZIP Phone For Persons Under 19 Years Old, Mother's Maiden Name Doctor's Name Allergies? Doctor's Address Emergency Contact Contact Phone Please complete the questions below for yourself or the person receiving the vaccine. No Yes Are you currently sick with a fever? No Yes Have you ever had a life threatening allergy to any component (or part) of the flu or pneumonia vaccine? If yes, please describe: No Yes Have you ever developed Guillain-Barre Syndrome within 6 weeks of receiving flu vaccine? No Yes Have you ever had a pneumonia shot? No Yes Are you a smoker or have a chronic medical condition such as asthma, heart or lung disease? If yes, please describe: No Yes Have you ever had a severe life threatening allergy to eggs or egg products? No Yes Are you currently pregnant? No Yes Do you have a history of asthma or wheezing? O No Yes Are you a child or adolescent receiving long-term aspirin therapy? No Yes Do you have a weakened immune system or have close contact with a person with an extremely weakened immune system who needs special care? No Yes Have you received any other vaccinations within the last 4 weeks? No Yes Have you taken an antiviral medication for the flu within the last 48 hours? Vaccine Trial Consent I have read, or had explained to me, the Vaccine Information Statement about trial vaccination. I have had a chance to ask questions, which were answered to my satisfaction, and I understand the benefits and risks of the vaccination as described. I request that the trial vaccination be given to me (or the person named above for whom I am authorized to make this request). I authorize the release of any medical or other information necessary to process a Medicare or other insurance claim or for other public health purpose. I have received a copy of the Patient Bill of Rights. Signature of Recipient (Parent or Guardian) DateStep by Step Solution
There are 3 Steps involved in it

Get step-by-step solutions from verified subject matter experts