

Question: Case Questions - Please answer all 4 question! 1. Why is patient experience a quality concern? Do you see this changing in the future? 2.
Case Questions - Please answer all 4 question!
1. Why is patient experience a quality concern? Do you see this changing in the future?
2. How can Bryce engage his boss and his peers heading other departments to work together in support of better patient experiences?
3. How does a focus on patient education help resolve some of the tensions noted in the case?
4. What additional steps can Bryce take to better align leaders and the administrative silos mentioned in this case?
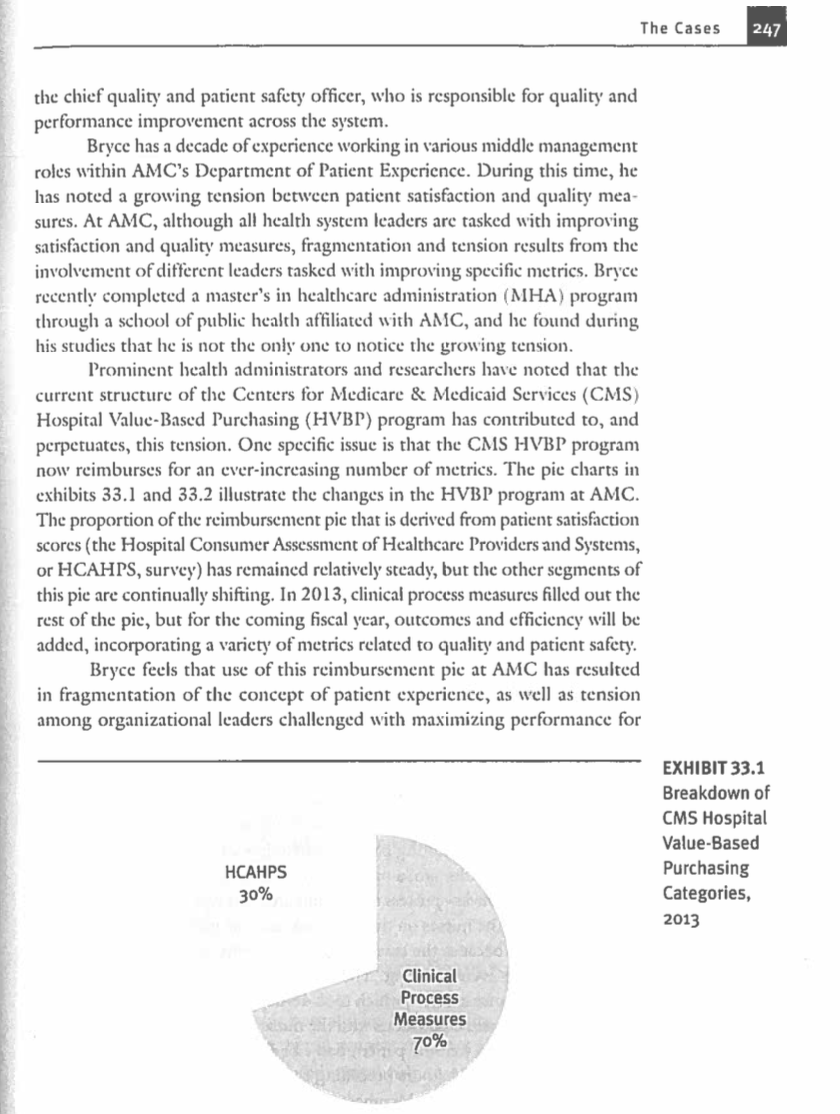
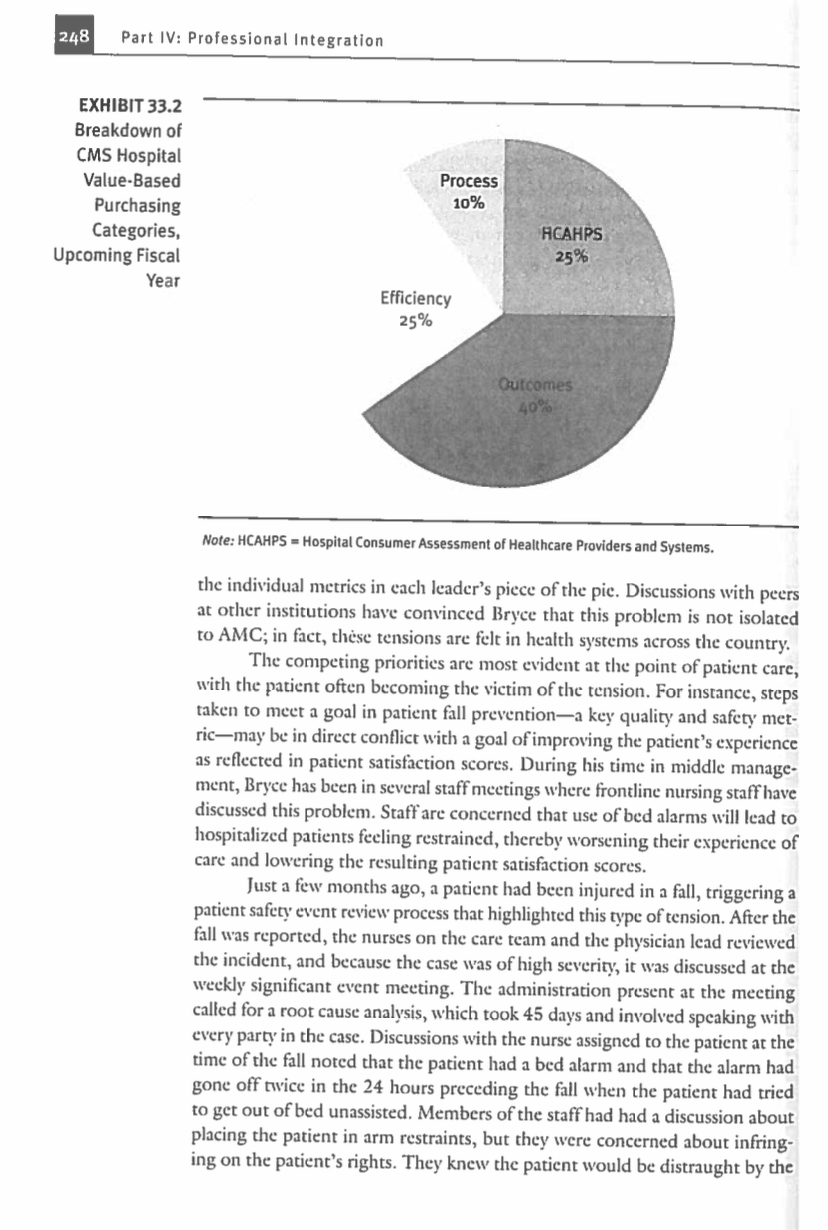
CASE 33 Managing the Patient Experience: Facing the Tension Between Quality Measures and Patient Satisfaction Jennifer Lynn Hefner, Susan Moffatt-Bruce, and Ann Scheck McAlearney B a ryce Jackson has recently been appointed chicf experience officer for Academic Medical Center (AMC), a large tertiary.care health system consisting of six hospitals with a total of 1,500 inpatient beds and an annual average of 60,000 discharges. In this role, he will oversee the Depart- ment of Patient Experience, which has responsibility for patient satisfaction data, patient family complaints/grievances, patient advocacy, volunteer services, information desks, and employee engagement. Bryce will report directly to The Cases 247 the chief quality and patient safety officer, who is responsible for quality and performance improvement across the system. Bryce has a decade of experience working in various middle management roles within AMC's Department of Patient Experience. During this time, he has noted a growing tension between patient satisfaction and quality mea- sures. At AMC, although all health system leaders are tasked with improving satisfaction and quality measures, fragmentation and tension results from the involvement of different leaders tasked with improving specific metrics. Bryce recently completed a master's in healthcare administration (MHA) program through a school of public health affiliated with AMC, and he found during his studies that he is not the only one to notice the growing tension. Prominent health administrators and researchers have noted that the current structure of the Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program has contributed to, and perpetuates, this tension. One specific issue is that the CMS HVBP program now reimburses for an ever-increasing number of metrics. The pic charts in exhibits 33.1 and 33.2 illustrate the changes in the HVBP program at AMC. The proportion of the reimbursement pic that is derived from patient satisfaction scores (the Hospital Consumer Assessment of Healthcare Providers and Systems, or HCAHPS, survey) has remained relatively steady, but the other segments of this pie are continually shifting. In 2013, clinical process measures filled out the rest of the pie, but for the coming fiscal year, outcomes and efficiency will be added, incorporating a variety of metrics related to quality and patient safety. Bryce feels that use of this reimbursement pic at AMC has resulted in fragmentation of the concept of patient experience, as well as tension among organizational leaders challenged with maximizing performance for EXHIBIT 33.1 Breakdown of CMS Hospital Value-Based Purchasing Categories, 2013 HCAHPS 30% Clinical Process Measures 70% 248 Part IV: Professional Integration EXHIBIT 33.2 Breakdown of CMS Hospital Value-Based Purchasing Categories, Upcoming Fiscal Year Process 10% HCAHPS 25% Efficiency 25% Outcomes 40% Note: HCAHPS - Hospital Consumer Assessment of Healthcare Providers and Systems. the individual metrics in each leader's piece of the pic. Discussions with peers at other institutions have convinced Bryce that this problem is not isolated to AMC; in fact, thse tensions are felt in health systems across the country. The competing priorities are most evident at the point of patient care, with the patient often becoming the victim of the tension. For instance, steps taken to meet a goal in patient fall preventiona key quality and safety met- ric-may be in direct conflict with a goal of improving the patient's experience as reflected in patient satisfaction scores. During his time in middle manage- ment, Bryce has been in several staff meetings where frontline nursing staff have discussed this problem. Staff are concerned that use of bed alarms will lead to hospitalized patients feeling restrained, thereby worsening their experience of care and lowering the resulting patient satisfaction scores. Just a few months ago, a patient had been injured in a fall, triggering a patient safety event review process that highlighted this type of tension. After the fall was reported, the nurses on the care team and the physician lead reviewed the incident, and because the case was of high severity, it was discussed at the weekly significant event meeting. The administration present at the meeting called for a root cause analysis, which took 45 days and involved speaking with every party in the case. Discussions with the nurse assigned to the patient at the time of the fall noted that the patient had a bed alarm and that the alarm had gone off twice in the 24 hours preceding the fall when the patient had tried to get out of bed unassisted. Members of the staff had had a discussion about placing the patient in arm restraints, but they were concerned about infring- ing on the patient's rights. They knew the patient would be distraught by the use of physical restraints, but they were under great time pressure and did not know if they would be able to have a prolonged discussion with the patient about the need to have both a safe and positive experience. Staff debate about the next course of action was ongoing when the patient suffered the injury fall. Based on this incident, and a variety of other prior experiences, Bryce has formed the opinion that much of the tension could be resolved through the devel- opment of a program to establish patient expectations. A recent large-scale survey rescarch study, which had been included on the reading list for his capstone MHA class, indicated that patients' "met" expectations were associated with their postvisit satisfaction scores--thus supporting Bryce's idea that managing expectations may be key to solving the problem. Bryce feels that, in the ambulatory setting, patients could be provided with information about what to expect as inpatients, includ- ing the needs of the hospital and its staff, to balance safety and satisfaction. This approach would be similar to airlines' efforts to emphasize flight attendants' roles in flight safety rather than just their roles in providing passenger service on board. Specifically, Bryce envisions appointing a multidisciplinary working group comprising all stakeholders to develop a Patient Expectation of Inpatient Care curriculum. The working group could develop an educational video to play on the hospital channel on the television in each inpatient bedroom. The video would directly present to patients the tension between satisfaction and safety and specifically highlight the recent patient fall case in which the debate over arm restraints was a factor. Each admitted patient could be directed to this video when they were assigned to a room. Bryce is confident that this approach could address the problems without involving the staff nurses directly in the cducation effort; nurses' direct involvement could be viewed as self-serving and would also add to their significant workload. Bryce views his new appointment as an opportunity to address tensions, build bridges, and knock down silos. Specifically, he feels that this new role, chief experience officer, is the ideal platform from which to implement his program of patient expectation management. However, despite his enthusiasm, Bryce realizes that he must prioritize his agenda and develop a long-term plan. Case Questions 1. Why is patient experience a quality concern? Do you see this changing in the future? 2. How can Bryce engage his boss and his peers heading other departments to work together in support of better patient experiences? 3. How does a focus on patient education help resolve some of the tensions noted in the case? 4. What additional steps can Bryce take to better align leaders and the administrative silos mentioned in this caseStep by Step Solution
There are 3 Steps involved in it
1 Expert Approved Answer
Step: 1 Unlock

Question Has Been Solved by an Expert!
Get step-by-step solutions from verified subject matter experts
Step: 2 Unlock
Step: 3 Unlock