

Question: I do Problem 4) There are two strategies (or therapies) for treating a particular disease. Strategy A is an operation that carries a risk of
I do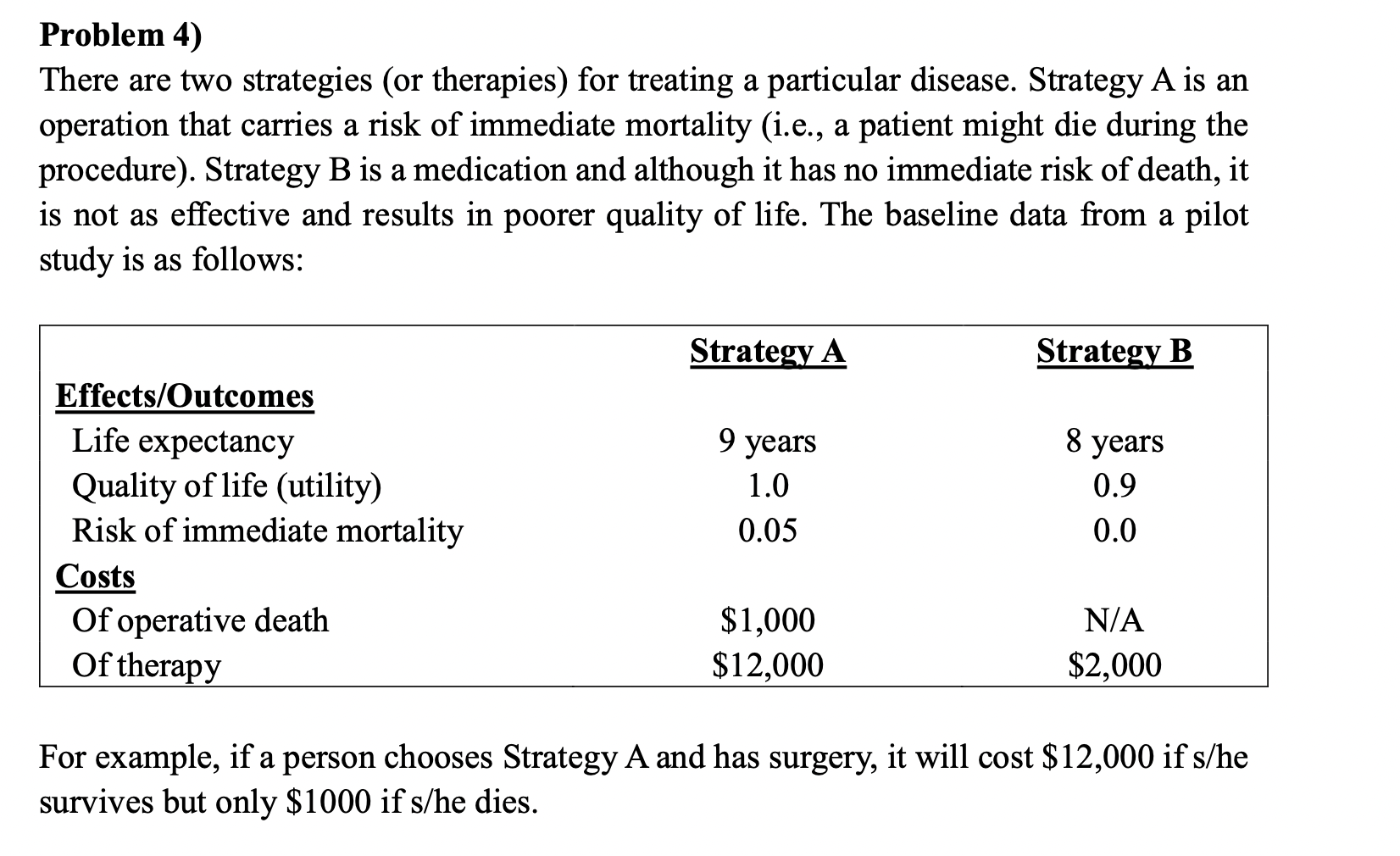
Problem 4) There are two strategies (or therapies) for treating a particular disease. Strategy A is an operation that carries a risk of immediate mortality (i.e., a patient might die during the procedure). Strategy B is a medication and although it has no immediate risk of death, it is not as effective and results in poorer quality of life. The baseline data from a pilot study is as follows: For example, if a person chooses Strategy A and has surgery, it will cost $12,000 if s/he survives but only $1000 if s/ he dies. a. Ranked by effectiveness, what are the costs, effects, and marginal cost-effectiveness ratios of the two therapies? b. From an effectiveness standpoint, at what risk of immediate mortality for Strategy A are the therapies equivalent? c. An important advantage of Strategy A is that quality of life is not impaired after surgery. Suppose this is not the case and Strategy A actually produces a decrement in quality of life. At what utility value for Strategy A do the interventions become equivalent? d. Suppose there are additional costs associated with Strategy B, such as long-term laboratory monitoring for toxicity. How much would Strategy B have to cost in order for Strategy A to become both cost- and life-saving? Problem 4) There are two strategies (or therapies) for treating a particular disease. Strategy A is an operation that carries a risk of immediate mortality (i.e., a patient might die during the procedure). Strategy B is a medication and although it has no immediate risk of death, it is not as effective and results in poorer quality of life. The baseline data from a pilot study is as follows: For example, if a person chooses Strategy A and has surgery, it will cost $12,000 if s/he survives but only $1000 if s/ he dies. a. Ranked by effectiveness, what are the costs, effects, and marginal cost-effectiveness ratios of the two therapies? b. From an effectiveness standpoint, at what risk of immediate mortality for Strategy A are the therapies equivalent? c. An important advantage of Strategy A is that quality of life is not impaired after surgery. Suppose this is not the case and Strategy A actually produces a decrement in quality of life. At what utility value for Strategy A do the interventions become equivalent? d. Suppose there are additional costs associated with Strategy B, such as long-term laboratory monitoring for toxicity. How much would Strategy B have to cost in order for Strategy A to become both cost- and life-saving
Step by Step Solution
There are 3 Steps involved in it

Get step-by-step solutions from verified subject matter experts