Question: Read del Monaco, C. & Volcker, J.P. (2004). Organization design for the breast service at Easter Medical Center. In A. R. Kovner and D. Neuhauser
Read
del Monaco, C. & Volcker, J.P. (2004). Organization design for the breast service at Easter Medical Center. In A. R. Kovner and D. Neuhauser (Eds.), Health services management: Readings, cases, and commentary (8th ed., pp. 248-252). Chicago: Health Administration Press.
The Organization Design for the Breast Service at Easter Medical Center case offers a summative opportunity to examine a health care organization that is struggling with true-life leadership challenges, some of which you might encounter at one time or another in your professional career as a health care leader or as a member of a health care team. You are completing Part I of the course project to demonstrate your ability to diagnose the current situation for the breast service at EMC and identify main problems/issues hindering the overall performance and strategic direction of the organization.
Last week, your group read the case, reviewed the course project, and posted to the group discussion board acknowledging such. This week, your group will complete the following:
Description of the situation (approximately 200 words).
Description of five main problems/issues with proposed causes (approximately 500 words).
Use the template provided to gather your data.
Note: You will reformat Part I in Week Six to be consistent with the required components and format of the final consulting report.
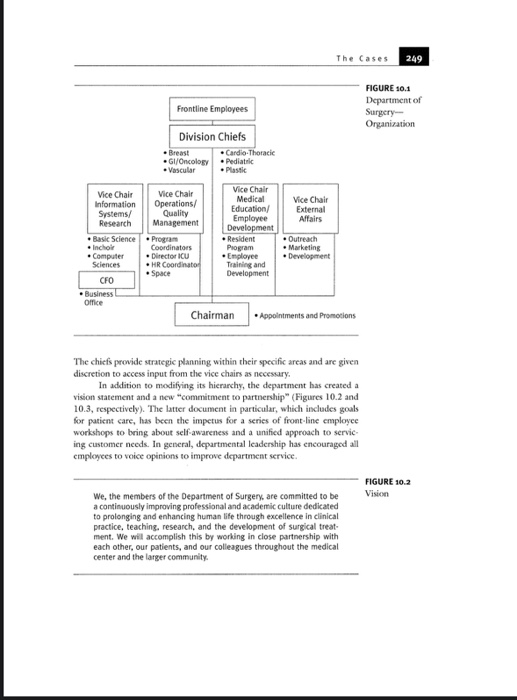




248 Professional integration Case 10 Organization Design for the Breast Service at Easter Medical Center Chiara del Monaco and James Paul Volcker Internal Issues: Background and Unit Organization Established in early 1992, the breast service seeks to deliver comprehensive care to women with breast discase. The service is a part of the Department of Surgery at Easter Medical Center (EMC), which over the last few years has undergone a wide reorganization focused primarily on information manage ment, operations, employee development, and marketing. The department feels that weaknesses in these areas have stifled its ability to provide quality service and, ultimately, increase market share. Tangible signs of the reorganization include a restructuring of the Department of Surgery (Figure 10.1). Physicians have been appointed as vice chairmen for information systems/research, operations/quality manage ment, medical education/employee development, and external affairs. These doctors are responsible to the department chairman for overseeing the re design of their respective areas. A chief financial officer supervises the business office in the department and provides financial guidance to the vice chairmen and division chiefs in their work. In addition, because physician autonomy and decision making are highly regarded as strengths in the department, a se ries of division chiefs remain as governors of their respective surgical services. The Cases 249 Frontline Employees FIGURE 10.1 Department of Surgery Organization Division Chiefs - Breast Cardio-Thoracic .Gl/Oncology Pediatric Vascular Plastic Vice Chair External Affairs Vice Chair Vice Chair Information Operations/ Systems/ Quality Research Management Basic Science Program Inchor Coordinators Computer Directoriu Sciences .HR Coordinator Space CFO Business Office Vice Chair Medical Education Employee Development Resident Program Employee Training and Development Outreach Marketing Development Chairman Appointments and Promotions The chiefs provide strategic planning within their specific arcas and are given discretion to access input from the vice chairs as necessary. In addition to modifying its hierarchy, the department has created a vision statement and a new "commitment to partnership" (Figures 10.2 and 10.3, respectively). The latter document in particular, which includes goals for patient care, has been the impetus for a series of front-line employee workshops to bring about self-awareness and a unified approach to service ing customer needs. In general, departmental leadership has encouraged all employees to voice opinions to improve department service FIGURE 10.2 Vision We, the members of the Department of Surgery, are committed to be a continuously improving professional and academic culture dedicated to prolonging and enhancing human life through excellence in clinical practice, teaching, research, and the development of surgical treat- ment. We will accomplish this by working in close partnership with each other, our patients, and our colleagues throughout the medical center and the larger community. 3 of 6 250 Professional Integration FIGURE 10.9 A Commitment We, the members of the Department of Surgery are committed to providing you to Partnership our patients, referring physicians, and colleagues throughout the medical center, with the highest quality service. We will endeavor to do this by holding ourselves to the following standards . We will respond to your inquiries and requests promptly, courteous and thoroughly . We will provide you with relevant comprehensive and timely information, . We wil listen carefully acknowledge your point of view, and encourage your questions so we may better understand your expectations. . We will engage you in a collaborative decision-making process to produce the best possible outcome. . We will work in close partnership with you and use all available resources to you might be experiencing . We will take the initiative to put you in direct and timely contact with the We will consistently demonstrate a willingness to meet your needs by going person who has the knowledge and experience to best serve you.. We will treat you with a depth of courtesy that demonstrates dignity empathy Sensitivity, and utmost respect for the diversity of those we serve It is a strength of the Department of Surgery that it has taken the steps to reorganize as it has. With the advent of managed care, the healthcare in dustry is no longer business as usual." Competitive pressures have generated the need for providers to focus not only on delivery of services, but also in creasingly on how those services are delivered. Iwees of efficiency within the industry have meant that outcomes assessment has become essential. The.com temporary healthcare provider needs to be able to monitor quality of service and have access to data through which to assess outcomes. These new needs have, in turn, required new types of training for the healthcare profesional The continuance of the division chic structure, with the separate sur gical services, is a potential weakness of the reorganization. In effect, the sur gical fiefdoms remain, governed by the service chiefs. Physician autonomy remains a feature of the department, at best, limited mechanisms of account ability exist within the new structure Mandating that the surgical services comply with the new way of doing things is nearly impossible yet it is crucial that the chiefs and the service physicians buy into the reorganization. They have to feel that the changes are positive steps in their work, or the hoped for improvements will not happen. Within this context of reorganization, the breast service has tended to maintain the status quo Nationally and internationally recognized physi cians whose collective reputation bring continuing business to the service via word-of-mouth recommendations he historically staffed the unit. Within 4 of 6 The Cases 251 this environment, new technology, competitive pricing, and operating of ciency are not deemed particularly mory, and the service has largely for felted opportunities to tap into the new departmental structure for mistance in modernizing praction. Consequently has to increase market share, hance long term profitability, or meet the needs of physician staff are not a tively planned for The breast service is ako handicapped by its own organizational design. Although physicians on the service report to the division chief, cach operates his or her practice independent. Whik the advantage of this arrangement is physician autonomy, this delivery design has many weaknesses. The first is high staff costs. Fach physician hires between one and three secretaries, whose responibilities include reception, billing, filing, ordering supplies, and scheduling operations and physician time. In addition, some physicians hire physician extenders (a registered nurse, nurse practitioner, or physician as- sistant) to provide addicional patient care le or no cross triation of functions exists-tasks are performed and passed on to the next compart ment. The sccond weakness is procedural inefficiency. The senior secretary determines the charges for physician service these charges are often arbitrary and have no relation to physician effort or practice costs. There is no strategy for the management of supplies/inventory, no standards of documentation for procedures, and no mechanism through which to monitor the quality of patient care. Third, the service staff is underdeveloped. Upon hiring, orienta tion to the EMC is perfunctory at best, and formal training in individual job responsibilities is nonexistent Office practices are passed along through word of-mouth, based on the way we've always donc it. The risk of perpetuating chroes is therefore great. In 1997, it was discovered that a content crror by a previous billing secretary had led to a large low of revenue for one physician practice. The wall does not have a cohesive view of what needs to be done Suall development and formalized processes are needed to improve services and reduce mistakes in the breast service. Each office recognizes the need to take such seeps, but lacks the necessary time. Heavy clinical responsibilities translate into physicians bring, at best, disinterested managers, with all of the ramifications that term implies Wcancies in the organization of the best service have been ex acerbated by a number of changes in physician personnel. Over a recent two- month period, the former service chief resigned and was replaced, one physician terminated her practice, and another has taken an indefinite leave of abuse. This staff redaction will represent a significant decrease in service revenues. Two remaining breastsurgeons are sharing the financial expenses of the unit. These two physicians have required the assistance of a recent graduate general surgeon to cover the wrow of patients. In addition of three plastic and reconstructive surgeois integral to the functioning of a comprehensive breast center, one has left, a sccond plans to leavc, and a third is incaperienced 252 Professional integration The unit can no longer function independently or compechensively. The lack of reconstructive surgery undermines the service's stated mission as a com prehensive breast center, forcing patients to go elsewhere for these services. External Issues: The Response to Change In addition to internal pressures, the breast service is facing external pressures as well. Under the management of the previous chicf, the service did not react to several environmental conditions that now make it les competitive in the local marketplace. Technical changes in the field have been rapidly advancing over the past two years to include a surgical procedure called sentinel lymph node biopsy and the use of the ABBI instrument for surgical trcatment of breast cancer. As of yet, however, the breast service has not made a resource commitment in terms of dollars or personnel to these new procedures Second, the era of information systems technology has been ignored The individual physician offices in the service continue to schedule appoint monts by hand. No integrated system, database collection, or outcomes mca surement mechanism exists. Last, the service does not, to date, align itself with any insurance carrier. Provider shifts have taken place within the man aged care industry, but the decision not to align endures. Breast service pa tients who decide to have surgery are informed by the secretary that they are responsible for investigating their own insurance benefits and for paying the remaining balance in its entirety. With the high costs of today's healthcare many patients are actively seeking competent physicians within provider net works. Breast service physicians believe that the wave of managed care will pass, favoring the traditional fee for service model. Although this remains to be soen, it does not mean that care should not be managed efficiently and costs contained. Maintaining a position in the marketplace requires knowing what it costs to care for patients Another issue to consider is the reaction of patients to the delivery of Care at the breast service. At present, enormous coordinated effort is necessary to take patients from scheduled appointments to the physician's consultation room, then into the hospital for surgery, and return them home satisfied with the services provided. Within this process are many pockets of incfficiency for staff and patients, resulting in delays and frustration every point in the process. Historically, most patients have accepted office incfficiencies out of great loyalty to their surgeon. The contemporary woman who seeks care for breast discase has many choices in this marketplace. The question is will the existing structure remain clinically respected and financially sound amidst the changing internal and external environment? Had the environment remained stable, the breast service might be able to perpetuate its existence with a low level of complexity. This possibility is no longer an option. The The Cases 253 breast center must adapt to its environment and upgrade the complexity of its goals, strategy, and structure to maintain viability in the local marketplace An organization with high complexity is more able to adapt to a changing environment, and adaptability is the key to survival. Week Five Course Project Submission: Easter Breast Service, Part 1 Group #: Names of group members: Part I Description of the situation: Main problems issues causes 11. 2 3 14 15. 248 Professional integration Case 10 Organization Design for the Breast Service at Easter Medical Center Chiara del Monaco and James Paul Volcker Internal Issues: Background and Unit Organization Established in early 1992, the breast service seeks to deliver comprehensive care to women with breast discase. The service is a part of the Department of Surgery at Easter Medical Center (EMC), which over the last few years has undergone a wide reorganization focused primarily on information manage ment, operations, employee development, and marketing. The department feels that weaknesses in these areas have stifled its ability to provide quality service and, ultimately, increase market share. Tangible signs of the reorganization include a restructuring of the Department of Surgery (Figure 10.1). Physicians have been appointed as vice chairmen for information systems/research, operations/quality manage ment, medical education/employee development, and external affairs. These doctors are responsible to the department chairman for overseeing the re design of their respective areas. A chief financial officer supervises the business office in the department and provides financial guidance to the vice chairmen and division chiefs in their work. In addition, because physician autonomy and decision making are highly regarded as strengths in the department, a se ries of division chiefs remain as governors of their respective surgical services. The Cases 249 Frontline Employees FIGURE 10.1 Department of Surgery Organization Division Chiefs - Breast Cardio-Thoracic .Gl/Oncology Pediatric Vascular Plastic Vice Chair External Affairs Vice Chair Vice Chair Information Operations/ Systems/ Quality Research Management Basic Science Program Inchor Coordinators Computer Directoriu Sciences .HR Coordinator Space CFO Business Office Vice Chair Medical Education Employee Development Resident Program Employee Training and Development Outreach Marketing Development Chairman Appointments and Promotions The chiefs provide strategic planning within their specific arcas and are given discretion to access input from the vice chairs as necessary. In addition to modifying its hierarchy, the department has created a vision statement and a new "commitment to partnership" (Figures 10.2 and 10.3, respectively). The latter document in particular, which includes goals for patient care, has been the impetus for a series of front-line employee workshops to bring about self-awareness and a unified approach to service ing customer needs. In general, departmental leadership has encouraged all employees to voice opinions to improve department service FIGURE 10.2 Vision We, the members of the Department of Surgery, are committed to be a continuously improving professional and academic culture dedicated to prolonging and enhancing human life through excellence in clinical practice, teaching, research, and the development of surgical treat- ment. We will accomplish this by working in close partnership with each other, our patients, and our colleagues throughout the medical center and the larger community. 3 of 6 250 Professional Integration FIGURE 10.9 A Commitment We, the members of the Department of Surgery are committed to providing you to Partnership our patients, referring physicians, and colleagues throughout the medical center, with the highest quality service. We will endeavor to do this by holding ourselves to the following standards . We will respond to your inquiries and requests promptly, courteous and thoroughly . We will provide you with relevant comprehensive and timely information, . We wil listen carefully acknowledge your point of view, and encourage your questions so we may better understand your expectations. . We will engage you in a collaborative decision-making process to produce the best possible outcome. . We will work in close partnership with you and use all available resources to you might be experiencing . We will take the initiative to put you in direct and timely contact with the We will consistently demonstrate a willingness to meet your needs by going person who has the knowledge and experience to best serve you.. We will treat you with a depth of courtesy that demonstrates dignity empathy Sensitivity, and utmost respect for the diversity of those we serve It is a strength of the Department of Surgery that it has taken the steps to reorganize as it has. With the advent of managed care, the healthcare in dustry is no longer business as usual." Competitive pressures have generated the need for providers to focus not only on delivery of services, but also in creasingly on how those services are delivered. Iwees of efficiency within the industry have meant that outcomes assessment has become essential. The.com temporary healthcare provider needs to be able to monitor quality of service and have access to data through which to assess outcomes. These new needs have, in turn, required new types of training for the healthcare profesional The continuance of the division chic structure, with the separate sur gical services, is a potential weakness of the reorganization. In effect, the sur gical fiefdoms remain, governed by the service chiefs. Physician autonomy remains a feature of the department, at best, limited mechanisms of account ability exist within the new structure Mandating that the surgical services comply with the new way of doing things is nearly impossible yet it is crucial that the chiefs and the service physicians buy into the reorganization. They have to feel that the changes are positive steps in their work, or the hoped for improvements will not happen. Within this context of reorganization, the breast service has tended to maintain the status quo Nationally and internationally recognized physi cians whose collective reputation bring continuing business to the service via word-of-mouth recommendations he historically staffed the unit. Within 4 of 6 The Cases 251 this environment, new technology, competitive pricing, and operating of ciency are not deemed particularly mory, and the service has largely for felted opportunities to tap into the new departmental structure for mistance in modernizing praction. Consequently has to increase market share, hance long term profitability, or meet the needs of physician staff are not a tively planned for The breast service is ako handicapped by its own organizational design. Although physicians on the service report to the division chief, cach operates his or her practice independent. Whik the advantage of this arrangement is physician autonomy, this delivery design has many weaknesses. The first is high staff costs. Fach physician hires between one and three secretaries, whose responibilities include reception, billing, filing, ordering supplies, and scheduling operations and physician time. In addition, some physicians hire physician extenders (a registered nurse, nurse practitioner, or physician as- sistant) to provide addicional patient care le or no cross triation of functions exists-tasks are performed and passed on to the next compart ment. The sccond weakness is procedural inefficiency. The senior secretary determines the charges for physician service these charges are often arbitrary and have no relation to physician effort or practice costs. There is no strategy for the management of supplies/inventory, no standards of documentation for procedures, and no mechanism through which to monitor the quality of patient care. Third, the service staff is underdeveloped. Upon hiring, orienta tion to the EMC is perfunctory at best, and formal training in individual job responsibilities is nonexistent Office practices are passed along through word of-mouth, based on the way we've always donc it. The risk of perpetuating chroes is therefore great. In 1997, it was discovered that a content crror by a previous billing secretary had led to a large low of revenue for one physician practice. The wall does not have a cohesive view of what needs to be done Suall development and formalized processes are needed to improve services and reduce mistakes in the breast service. Each office recognizes the need to take such seeps, but lacks the necessary time. Heavy clinical responsibilities translate into physicians bring, at best, disinterested managers, with all of the ramifications that term implies Wcancies in the organization of the best service have been ex acerbated by a number of changes in physician personnel. Over a recent two- month period, the former service chief resigned and was replaced, one physician terminated her practice, and another has taken an indefinite leave of abuse. This staff redaction will represent a significant decrease in service revenues. Two remaining breastsurgeons are sharing the financial expenses of the unit. These two physicians have required the assistance of a recent graduate general surgeon to cover the wrow of patients. In addition of three plastic and reconstructive surgeois integral to the functioning of a comprehensive breast center, one has left, a sccond plans to leavc, and a third is incaperienced 252 Professional integration The unit can no longer function independently or compechensively. The lack of reconstructive surgery undermines the service's stated mission as a com prehensive breast center, forcing patients to go elsewhere for these services. External Issues: The Response to Change In addition to internal pressures, the breast service is facing external pressures as well. Under the management of the previous chicf, the service did not react to several environmental conditions that now make it les competitive in the local marketplace. Technical changes in the field have been rapidly advancing over the past two years to include a surgical procedure called sentinel lymph node biopsy and the use of the ABBI instrument for surgical trcatment of breast cancer. As of yet, however, the breast service has not made a resource commitment in terms of dollars or personnel to these new procedures Second, the era of information systems technology has been ignored The individual physician offices in the service continue to schedule appoint monts by hand. No integrated system, database collection, or outcomes mca surement mechanism exists. Last, the service does not, to date, align itself with any insurance carrier. Provider shifts have taken place within the man aged care industry, but the decision not to align endures. Breast service pa tients who decide to have surgery are informed by the secretary that they are responsible for investigating their own insurance benefits and for paying the remaining balance in its entirety. With the high costs of today's healthcare many patients are actively seeking competent physicians within provider net works. Breast service physicians believe that the wave of managed care will pass, favoring the traditional fee for service model. Although this remains to be soen, it does not mean that care should not be managed efficiently and costs contained. Maintaining a position in the marketplace requires knowing what it costs to care for patients Another issue to consider is the reaction of patients to the delivery of Care at the breast service. At present, enormous coordinated effort is necessary to take patients from scheduled appointments to the physician's consultation room, then into the hospital for surgery, and return them home satisfied with the services provided. Within this process are many pockets of incfficiency for staff and patients, resulting in delays and frustration every point in the process. Historically, most patients have accepted office incfficiencies out of great loyalty to their surgeon. The contemporary woman who seeks care for breast discase has many choices in this marketplace. The question is will the existing structure remain clinically respected and financially sound amidst the changing internal and external environment? Had the environment remained stable, the breast service might be able to perpetuate its existence with a low level of complexity. This possibility is no longer an option. The The Cases 253 breast center must adapt to its environment and upgrade the complexity of its goals, strategy, and structure to maintain viability in the local marketplace An organization with high complexity is more able to adapt to a changing environment, and adaptability is the key to survival. Week Five Course Project Submission: Easter Breast Service, Part 1 Group #: Names of group members: Part I Description of the situation: Main problems issues causes 11. 2 3 14 15


