New Semester
Started
Get
50% OFF
Study Help!
--h --m --s
Claim Now
Question Answers
Textbooks
Find textbooks, questions and answers
Oops, something went wrong!
Change your search query and then try again
S
Books
FREE
Study Help
Expert Questions
Accounting
General Management
Mathematics
Finance
Organizational Behaviour
Law
Physics
Operating System
Management Leadership
Sociology
Programming
Marketing
Database
Computer Network
Economics
Textbooks Solutions
Accounting
Managerial Accounting
Management Leadership
Cost Accounting
Statistics
Business Law
Corporate Finance
Finance
Economics
Auditing
Tutors
Online Tutors
Find a Tutor
Hire a Tutor
Become a Tutor
AI Tutor
AI Study Planner
NEW
Sell Books
Search
Search
Sign In
Register
study help
business
financial management theory
Gapenski's Healthcare Finance An Introduction To Accounting And Financial Management 7th Edition Kristin L. Reiter, Paula H. Song - Solutions
Why is the number of members so important in a capitated environment?
Explain this statement: “To minimize financial risk, match the cost structure to the revenue structure.”
What cost structure would minimize risk if a provider had all feefor-service reimbursement?
What cost structure would minimize risk if a provider were entirely capitated?
What are real-world constraints on creating matching cost structures?
Explain the differences between fixed costs and variable costs.
What components make up total costs?
a. What is cost-volume-profit (CVP) analysis?b. Why is it so useful to health services managers?
a. Define contribution margin.b. What is its economic meaning?
a. Write out and explain the equation for volume breakeven.b. What role does contribution margin play in this equation?
What elements of profit analysis change when a provider moves from a fee-for-service to a discounted fee-for-service environment?
What are the critical differences in profit analysis when it is conducted in a capitated environment versus a fee-for-service environment?
How do provider incentives differ when the provider moves from a fee-for-service to a capitated environment?
a. What cost structure is best when a provider is primarily capitated? Explain.b. What cost structure is best when a provider is reimbursed primarily by fee-for-service? Explain.
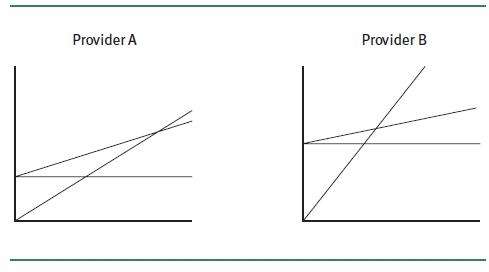
Consider the CVP graphs below for two providers operating in a fee-for-service environment:a. Assuming the graphs are drawn to the same scale, which provider has the greater fixed costs? The greater variable cost rate? The greater per unit revenue?b. Which provider has the greater contribution
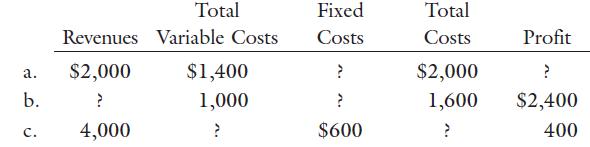
Consider the data in the table below for three independent health services organizations:Fill in the missing data indicated by question marks. Total Fixed Total Revenues Variable Costs Costs Costs Profit a. $2,000 $1,400 ? $2,000 ? b. 1,000 2 1,600 $2,400 C. 4,000 ? $600 ? 400
Assume that a radiologist group practice has the following cost structure:Furthermore, assume that the group expects to perform 7,500 procedures in the coming year.a. Construct the group’s base case projected P&L statement.b. What is the group’s contribution margin? What is its accounting
General Hospital, a not-for-profit acute care facility, has the following cost structure for its inpatient services:The hospital expects to have a patient load of 15,000 inpatient days next year.a. Construct the hospital’s base case projected P&L statement.b. What is the hospital’s
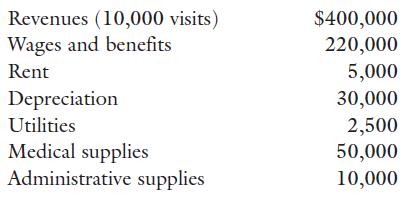
You are considering starting a walk-in clinic. Your financial projections for the first year of operations are as follows:Assume that all costs are fixed, except supply costs (medical and administrative), which are variable. Furthermore, assume that the clinic must pay taxes at a 30 percent rate.a.
Review the walk-in clinic data presented in problem 5.5. Construct projected P&L statements at volume levels of 8,000, 9,000, 10,000, 11,000, and 12,000 visits.a. Assume that the base case forecast is 10,000 visits. What is the clinic’s degree of operating leverage (DOL) at this volume level?
Triangle Health Center currently provides 1,000 visits per year at a price of $50 per visit. The variable cost per visit (variable cost rate)is $30, and total fixed costs are $15,000. The business manager suggests that Triangle Health Center can increase the number of visits to 1,200 per year by
Charity Hospital, a not-for-profit, has a maximum capacity of 15,000 discharges per year. Variable patient service costs are $495 per discharge. Variable general and administrative costs are $5 per discharge. Fixed hospital overhead costs are $4,000,000 per year.The current reimbursement rate is
What is the difference between direct and indirect costs?
Give several examples of indirect and direct costs for a hospital’s emergency services department.
What is meant by the term cost allocation? By the term full costs?
What is the goal of cost allocation?
Why is cost allocation important to health services managers?
What are the definitions of a cost pool, a cost driver, and an allocation rate?
Under what conditions should a single overhead department be divided into multiple cost pools?
On what theoretical basis are cost drivers chosen?
What two characteristics make an effective cost driver?
What are the four steps in the cost allocation process?
Explain how they differ.
Which method do you think is the most accurate? Which is the least accurate?
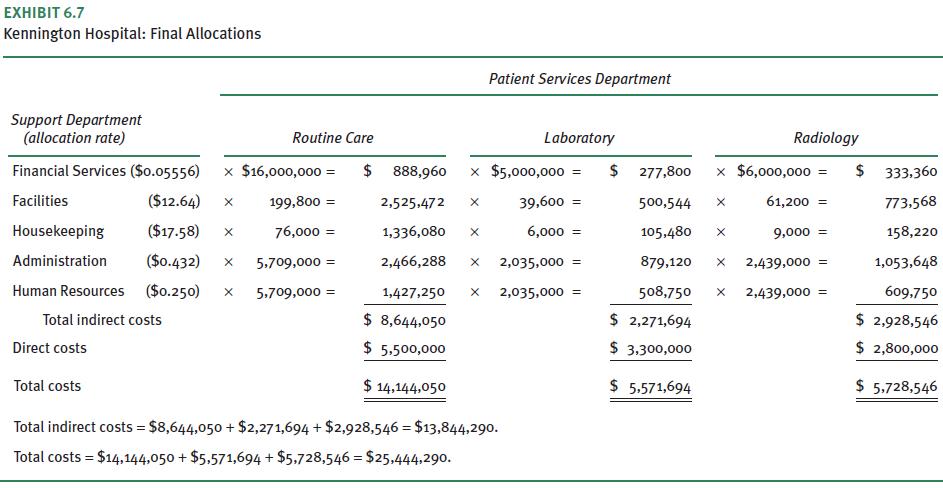
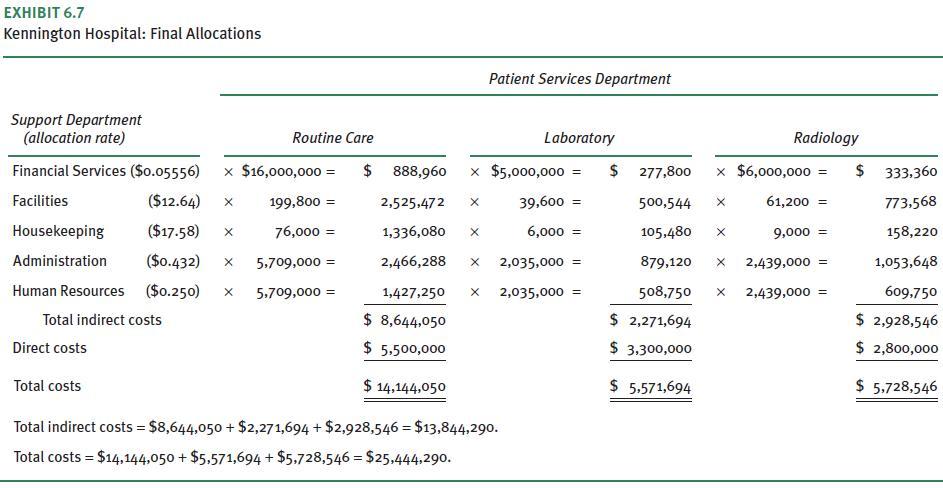
Briefly outline the allocation procedures used by Kennington Hospital.
What underlying characteristic creates a good cost driver?
What are the two properties of an effective cost driver?
What is the most important organizational benefit derived from the selection of an effective cost driver?
What are the advantages of changing from a poor cost driver to a better one?
What are the costs involved in the change?
Why is good cost allocation critical to good decision-making?
What are the two primary tests that good cost allocation processes pass?
Why is the cost allocation process important to health services managers?
What are the primary differences between direct and indirect costs?
a. What are the three primary methods of cost allocation?b. What are the differences among them?
a. What is a cost pool?b. What is a cost driver?c. How is the cost allocation rate determined?
Under what circumstances should an overhead department be divided into multiple cost pools?
Effective cost drivers, and the resulting allocation system, must have what two important attributes?
Briefly describe (illustrate) the cost allocation process. (To keep things simple, use the direct method for your illustration.)
The housekeeping services department of Ruger Clinic, a multispecialty practice, had $100,000 in direct costs in 2020.These costs must be allocated to Ruger’s three revenue-producing patient services departments using the direct method. Two cost drivers are under consideration: patient services
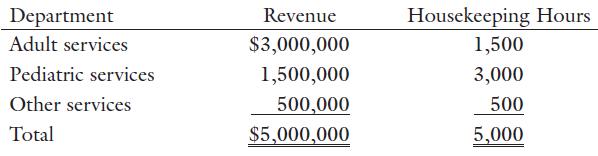
Refer to problem 6.1. Assume that the three patient services departments are adult services, pediatric services, and other services.The patient services revenue and hours of housekeeping services for each department are as follows:a. What is the dollar allocation to each patient services department
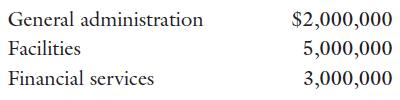
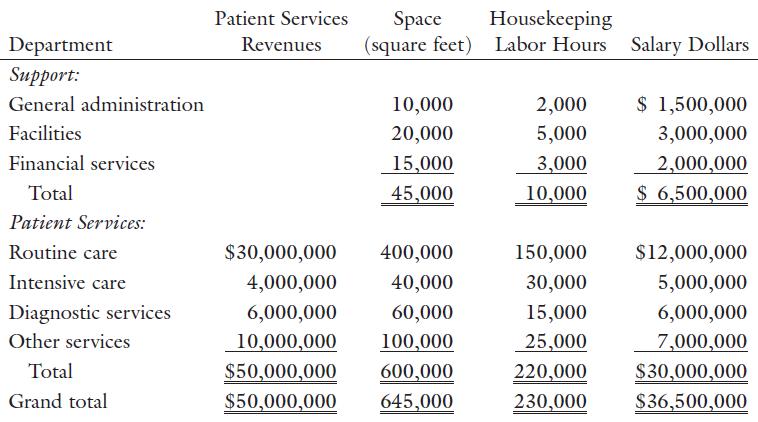
Assume that the hospital uses the direct method for cost allocation.Furthermore, the cost driver for general administration and financial services is patient services revenue, while the cost driver for facilities is space utilization.a. What are the appropriate allocation rates?b. Use an allocation
Assume that the hospital uses salary dollars as the cost driver for general administration, housekeeping labor hours as the cost driver for facilities, and patient services revenue as the cost driver for financial services. (The majority of the costs of the facilities department stem from the
Now assume that the hospital uses the step-down method for cost allocation, with salary dollars as the cost driver for general administration, housekeeping labor hours as the cost driver for facilities, and patient services revenue as the cost driver for financial services. Assume also that the
Return to the direct method of cost allocation and use the same cost drivers as specified in problem 6.4 for the general administration and facilities departments. However, assume that $2,000,000 of financial services costs is related to billing and managerial reporting and $1,000,000 is related to
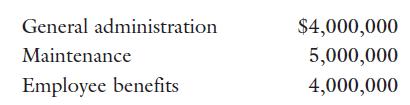
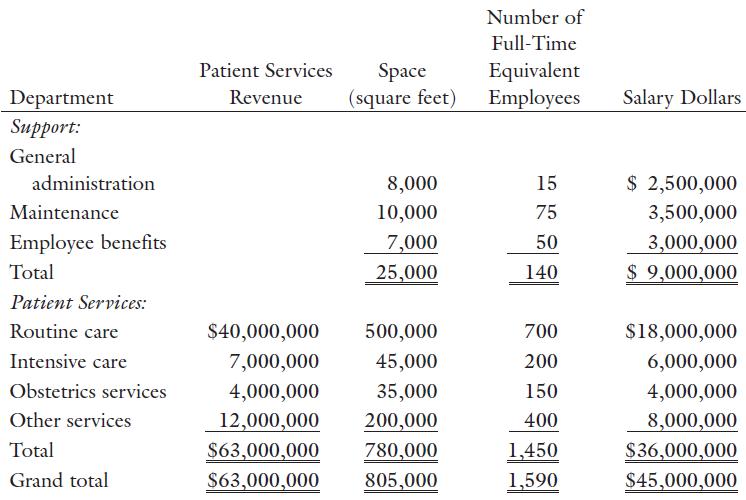
Assume the hospital uses the direct method for cost allocation.Furthermore, the cost driver for general administration is patient services revenue, the cost driver for maintenance is space utilization, and the cost driver for employee benefits is the number of full-time equivalent employees.a. What
Assume that the hospital uses salary dollars as the cost driver for general administration and employee benefits, and space utilization as the cost driver for maintenance.a. What are the appropriate allocation rates?b. Use an allocation table similar to exhibit 6.7 to allocate the hospital’s
Briefly describe the following service costing methods:a. Cost-to-charge ratio (CCR)b. Relative value unit (RVU)c. Activity-based costing (ABC)
Explain how time-driven activity-based costing (TDABC) differs from the other three methods.
What is the difference between a price taker and a price setter?
Are healthcare providers generally price takers or price setters exclusively? Explain your answer.
Describe two common pricing strategies used by price setters and their implications for financial survivability.
Is cross-subsidization used by providers as frequently today as it was in the past? If not, why?
What is its greatest value?
Briefly explain the conceptual process for pricing individual services.
What do you think the price should be on Windsor’s new service?Justify your answer.
Briefly explain why the base case analysis required the calculation to move up the P&L statement rather than down (the normal direction).
How are capitated revenue requirements typically expressed?
What is scenario analysis, and why is it so critical to good pricing decisions?
What is the most uncertain variable in MMC’s capitated plan pricing analysis?
Describe the following methods used to estimate the cost of individual services:a. Cost-to-charge ratio (CCR) methodb. Relative value unit (RVU) methodc. Activity-based costing (ABC) method
What is the time-driven activity-based costing method (TDABC), and how does it differ from the methods listed in question 7.1?Question 7.1Describe the following methods used to estimate the cost of individual services:a. Cost-to-charge ratio (CCR) methodb. Relative value unit (RVU) methodc.
a. Using a medical group practice to illustrate your answer, explain the difference between a price setter and a price taker.b. Can most providers be classified strictly as either a price setter or a price taker?
Explain the essential differences between full cost pricing and marginal cost pricing strategies.
What would happen financially to a health services organization over time if its prices were set at:a. Full costs?b. Marginal costs?
a. What is cross-subsidization (price shifting)?b. Is it as prevalent today as it has been in the past?
a. What is target costing?b. Suppose a hospital was offered a capitation rate for a covered population of $40 per member per month (PMPM). Briefly explain how target costing would be applied in this situation.
What is the role of accounting information in pricing decisions?
a. What is scenario analysis as applied to pricing decisions?b. Why is it such an important part of the process?
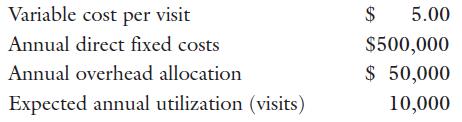
Assume that the managers of Fort Winston Hospital are setting the price for a new outpatient service. Here are relevant data estimates:a. What per visit price must be set for the service to break even? To earn an annual profit of $100,000?b. Repeat parta, but assume that the variable cost per visit
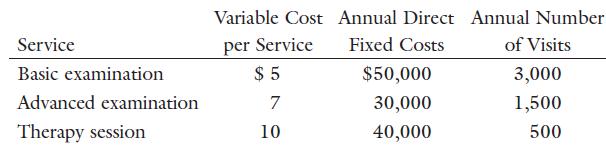
The audiology department at Randall Clinic offers many services to the clinic’s patients. The three most common, along with cost and utilization data, are as follows:a. What is the fee schedule for these services, assuming that the goal is to cover only variable and direct fixed costs?b. Assume
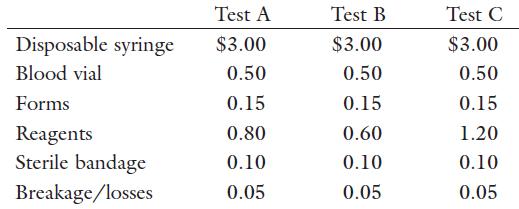
Allied Laboratories is combining some of its most common tests into one-price packages. One such package will contain three tests that have the following variable costs:When the tests are combined, only one syringe, form, and sterile bandage will be used. Furthermore, only one charge for
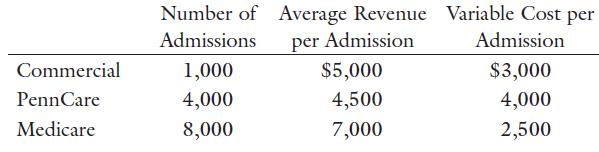
Assume that Valley Forge Hospital has only the following three payer groups:The hospital’s fixed costs are $38 million.a. What is the hospital’s net income?b. Assume that half of the 100,000 covered lives in the commercial payer group will be moved into a capitated plan. All utilization and
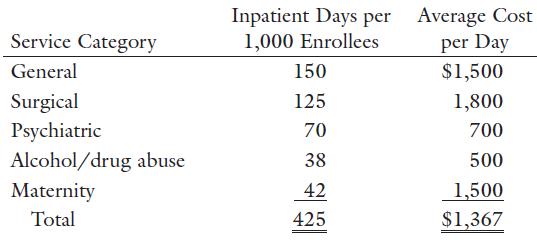
Bay Pines Medical Center estimates that a capitated population of 50,000 would have the following base case utilization and total cost characteristics:In addition to medical costs, Bay Pines allocates 10 percent of the total premium (total capitated revenue) for administration/reserves.a. What is
Assume that a primary care physician practice performs only physical examinations. However, there are three levels of examination—I, II, and III—that vary in depth and complexity.An RVU analysis indicates that a level I examination requires 10 RVUs, a level II exam 20 RVUs, and a level III exam
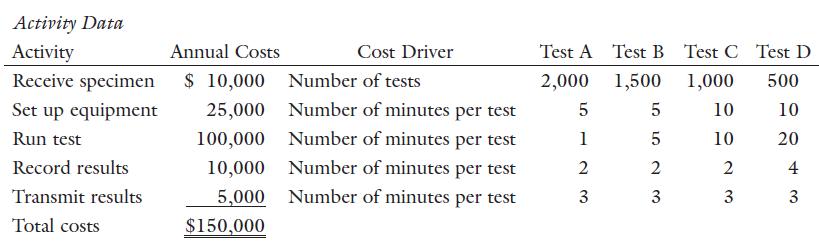
Consider the following data for a clinical laboratory:a. Using ABC techniques, determine the cost allocation rate for each activity.b. Now, using these allocation rates, estimate the total cost of performing each test.c. Verify that the total annual costs aggregated from individual test costs equal
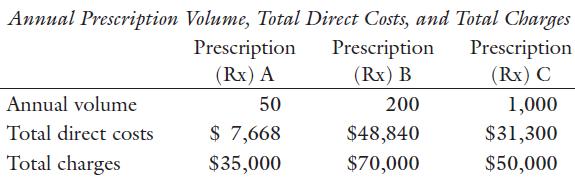
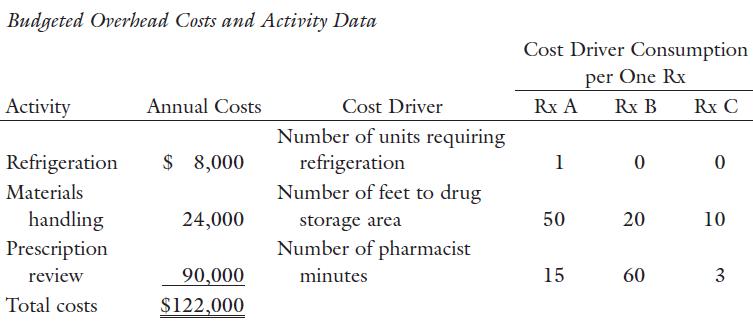
A hospital pharmacy fills three types of prescriptions. Prescription A requires refrigeration to maintain the drug’s activity. Prescription B has potentially fatal interactions with other drugs and therefore requires careful review by a pharmacist. Prescription C is a basic, common drug that
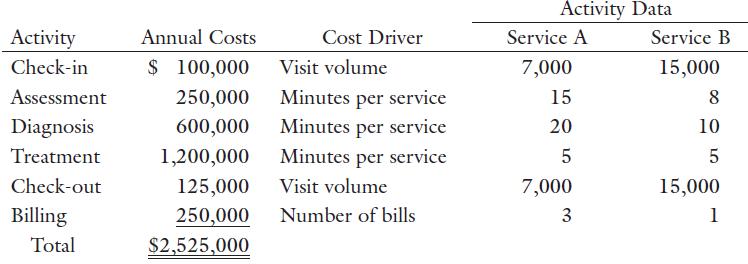
Consider the following data for a primary care practice that provides two types of services, A and B:a. Using ABC techniques, determine the allocation rate for each overhead activity.b. Determine the overhead costs per visit for each type of service.c. Verify that the total annual costs aggregated
Briefly describe the nature and use of the following corporate planning tools:a. Strategic planb. Values statementc. Mission statementd. Vision statement
Briefly describe the contents of a typical financial plan.
What is budgeting?
What are its primary purposes and benefits?
What time periods are used in budgeting?
What are the primary differences between conventional budgets and zero-based budgets?
What are the primary differences between top-down budgets and bottom-up budgets?
What are some of the budget types used within health services organizations?
Briefly describe the purpose and use of each.
How are the statistics budget, revenue and expense budgets, and operating budget related?
What are some of the key assumptions required to prepare an operating budget?
Do the required assumptions depend on the type of organization and the nature of its reimbursement contracts?
Showing 1700 - 1800
of 2201
First
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
Step by Step Answers