Question: 574 Capstone Cases Cause Caus CAPSTONE CASE E: QUALITY OF CARE IN SEVEN BOSTON HOSPITALS wat is actually done to the patient, that is the
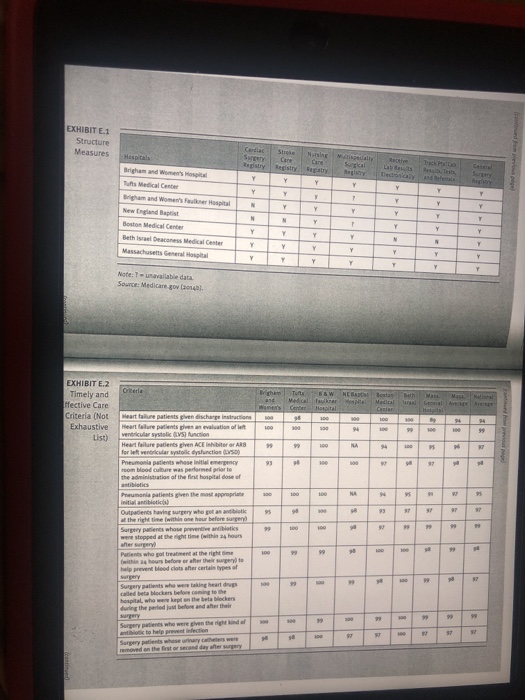
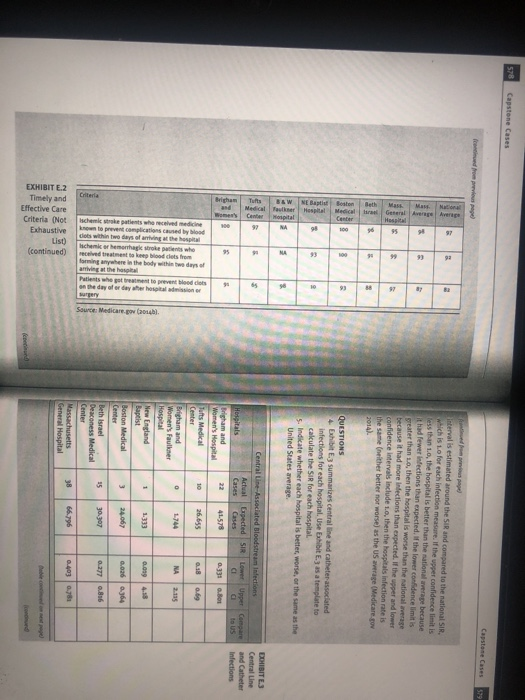
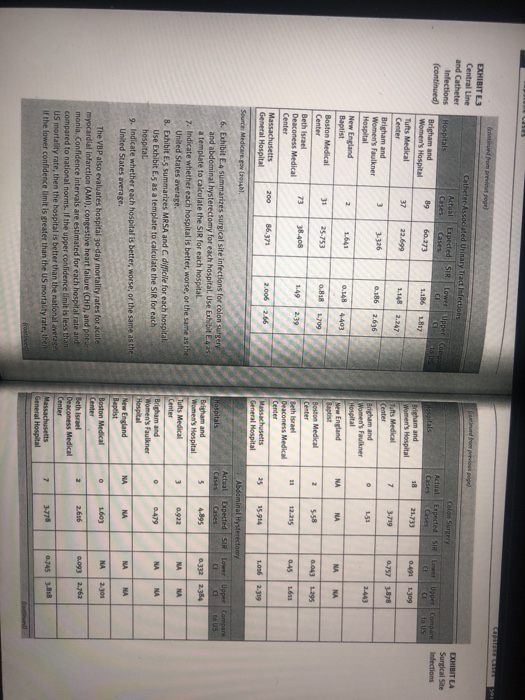
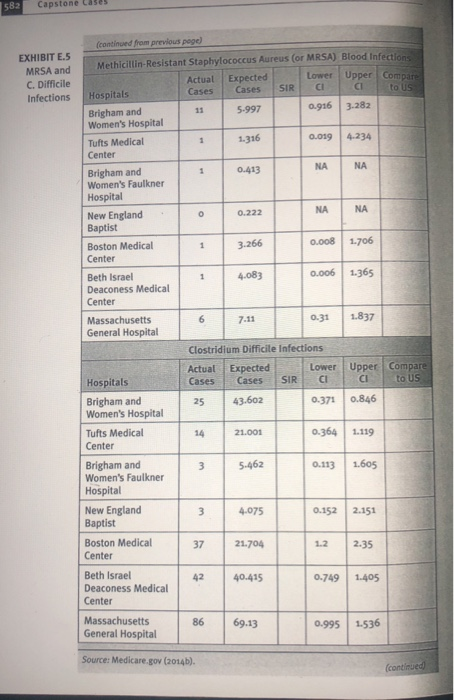
574 Capstone Cases Cause Caus CAPSTONE CASE E: QUALITY OF CARE IN SEVEN BOSTON HOSPITALS wat is actually done to the patient, that is the sequence and coordi sation of activities. These include the technical aspects of care, or the scence of care activities of professionals well as the interper sonal spects of care or the art of caree, how patients are treated Process measures tend to be easier to collect the outcome measures Sess time dependent, and less dependent on peuve patient follow The medical record does track some but not all aspects of process of care. Process of care measures do depend on agreed upon criteria for care. Outcome measures refer to the changes in health status as a result of care. It is multidimensional and may include peal health status indicators as well as adverse outcomes of care such as Infections, complications, mortality and reasons. By Steven T. Reming The Affordable Care Acted a hospital value-based puh (VEP) program at the Centers for Medicare & Medical Services that rewards acute care hospitals with incentive payments for the y of care they provide to Medicare patients. The Hospital com program collects various structure, process, and outcome Indian for quality of care that are used by the VS gram. Thische compares seven Boston hospitals inters of these indicat Brigham and Women's Hospital is a bed teaching her associated with the Harvard Medical School atrak quality of medical care and has deep historical carly nineteenth century Brigham and Women's 3150-bed community teaching hospital founded in onda in southwest Boston Tufts Medical Center is 345-bed pital amiliated with Tufts School of Medicine and located Boston. New England Baptist hospitalisa-bed hospital with national reputation for the treatment of orthopedic and musculos etal conditions. Boston Medical Center is a 496-bed academic del center location in the South End neighborhood of Boston, Beth Deaconess Hospital is an 8-bed teaching hospital associated with the Harvard Medical School, Massachusetts General Hospital is the larg est and oldest hospital in New England. It is a so-bed medical center consistently ranked highly on the quality of care and reputation of the 16 clinical specialties Avedis Donabedian (1980) has proposed that quality of care be measured along three different dimensions: structure, process and outcome. Measures of structure relate to personnel, facilities and their configurations. Indicators such as fire code compliance, bacity cleanliness, physician licensure, and the ratio of RNs to total nurses would be considered measures of structure. This information is ready obtained from existing documents and inspection reports. One mar disadvantage of these measures is the assumption that the capacity to provide care structure) translates into the actual processes of which translates into favorable outcomes. Process measures refer to QUESTIONS 1. NE.slist seven structure measures for the seven Boston hospitals, which hospitals lack some measures that are presumably indicative of the capacity to provide care! 2. Bibit Lisa on haustive list of some process of care measures used by the VP. These measures we criteris deemed to be important for patient care. They document the percent of a sample of patients in which each measure is satisfied compared to Massachusetts and national averages. Why are these measures called process of care measures? 3. Compare Brigham and Women's Hospital to state and national Healthcare-associated infections are diverse outcomes of Care that are presumably associated with quality. These measures use a standardized infection ratio (SIR) to adjust for differences in the characteristics of patients using the hospital. They take into account type of patient care location, procedure, number of patients admitted with methicillin-resistant Staphylococcus (MRSA) or Cafe laboratory methods, hospital affiliation with a medical school, and bedste of the patient care location. The si is somewhat similar to the standardered mortality ratio (SMR) of the Indirect method of age adjusted mortality in that we calculate the expected number of infec. ons based on national benchmarks and adjustments. A confidence EXHIBIT E 1 Structure Measures Candia Bedstry Care Sora Debos Y Tufts Medical Center Y Y Y Y T Y Y Y 7. Y N Y Y Y Y Y Y Y N New England Bart Boston Medical Center Beth Deacon Medical N Y Y 1 Y Y Y Y Y Y Y Y Y y Y Y Y Y Y Y Y Y Y Y Note:?table data Source: Medicare gou Coul ant Mais EXHIBIT E.2 Timely and ffective Care Criteria (Not Exhaustive List) Tunts B&W NEB Best Bath Center Mortal Center 94 *** 94 + 0 100 Heart failure patients en discharge Heart failure patients gives an evaluation of left ventricular systoli VS) Action Heart failure patients given ACE ARB for left ventricular systolic dysfunction (SO) Pneumonia patients whose initial emergency room blood culture was performed prior to the administration of the hospital dose of ++ 99 94 95 AT 2 NA 95 * 95 37 Pneumonia patients given the most appropriate Initial antibiotic Outpatients having surgery who got an antibiotik at the right time with one hour before surgery Surgery in whose preventive antibiotics were stopped at the right time within 24 hours 99 100 99 Patients who got treatment at the right with 4 hours before or after the surgery to help prevent blood clots after certain types of 3 8 3 3 Surgery patients who were taking heart drugs called Bret Hackers before coming to the hospital, who were on the beachers during the periods before and after their Surgery patients who were given the right and of to help prevention Surgery patients whose nary catheters were removed on the Best or second day after surgery . 9 9 37 578 Capstone Cases Capstone Cases 529 18 82 Interval is estimated around the SIR and compared to the national SIR, which is to for each infection are. If the upper confidence limit is less than 1.0, the hospital is better than the national average because it had fewer Infections than expected. If the lower confidence it is greater than 1.0, then the hospital is worse than the nationale because it had more infections than expected. If the upper and lower confidence intervals include 1o, then the hospitals infection rate is the same neither better or worse) as the US average (Medicare. 2 2014). 8 3 16 QUESTIONS Exhibit E.3 summarizes central line and catheter associated infections for each hospital. Use Exhibit E.3 as a template to calculate the SIR for each hospital 5. Indikate whether each hospital is better worse, or the same as the United States average 6 2 2 & DDHIBITE.3 Central Line and Catheter Infections Put 16 Mass 98 90 Hospit Beth Mass Center B&W NE Baptist Boston Hospital NA MA Tufts 95 Brigha Ischemic stroke patients who received medicine known to prevent complications caused by blood cols within two days of anting at the hospital Hichem or hemorrhagle stroke received treatment to whe forming anywhere in the body within two doo Patients who got treatment to prevent blood com of or day her hospitali on the day of List) EXHIBIT 2 Timely and Effective Care Criteria (Not Exhaustive (continued) ker Hospital Medical General Ave arriving at the who Central Line-Associated Bloodstream Infections Actual Expected SIR Lower Upper Compare Hospitals Cases CI to US Brigham and 41.578 Women's Hospital 0.331 0.81 Tufts Medical 10 26.655 0.18 0.69 Center Brigham and 0 1.744 NA 2.135 Women's Faulkner Hospital New England 1 1.333 0.019 4.58 Baptist Boston Medical 3 24.067 0.06 0.364 Center Beth Israel 15 30.307 0.277 0.816 Deaconess Medical Sows MedicareGo Center Massachusetts General Hospital 38 66.796 0.403.7 EXHIBIT L3 Central Line and Catheter Infections (continued EXHIBIT LA Surgical Site Infections Actual Cases 89 pected SIR Lower User Compare . CI to US 21.733 0.491 1.309 18 7 3.719 0.757-88 3 2.66 Catheter Associated Urinary Tract Infections Actual Expected Sir Lower Upper Compa Hospitals Cases Cases CI Brigham and Women's Hospital 60.273 1.186 1.817 Tufts Medical 37 22.699 Center Brigham and 3-326 0.186 Women's Faulkner Hospital New England 1.641 0.148 Baptist 4403 Boston Medical 31 25.753 0.88 1709 Center Beth Israel 73 38.408 2.39 Deaconess Medical Center Massachusetts 200 86.373 2.006 2.66 General Hospital Brigham and Women's Hospital Tufts Medical Center Brigham and Women's Faulkner Hospital New England L53 2.443 N NA NA NA NA 2 5-58 0.043 1395 19 12.215 Boston Medical Center Beth Israel Deaconess Medical Center Massachusetts General Hospital 1.6 0:45 25 15-914 1.056 2.39 Source Medicare.gov Ch. Abdominal Hysterectomy Actual Expected SIR Lower Upper Compare a to US 5 4.895 0.332 2384 3 0.922 NA NA 6. Exhibit E4 summarizes surgical site infections for colon Surgery and abdominal hysterectomy for each hospital. Use Exhibit 425 a template to calculate the SiR for each hospital 7. Indicate whether each hospital is better, worse, or the same as the United States average. 8. Exhibit E.5 summarizes MRSA and C difficile for each hospital, Use Exhibit E.5 as a template to calculate the SIR for each hospital 9. Indicate whether each hospital is better, worse, or the same as the United States average. 0 0.419 NA NA Hospitals Brigham and Women's Hospital Tufts Medical Center Brigham and Women's Faulkner Hospital New England Baptist Boston Medical Center Beth Israel Deaconess Medical Center Massachusetts General Hospital NA NA NA NA 1.603 NA 2.301 2 2.616 The VBP also evaluates hospital 30-day mortality rates for acute myocardial infarction (AMI), congestive heart failure (CHF), and new monia. Confidence intervals are estimated for each hospital rate and compared to national norms. If the upper conlidence limit is less than US mortality rate, then the hospital is better than the national average if the lower confidence limit is greater than the US mortality rate, then 0.093 2.763 7 0.745.818 582 Capstone Cases 1 NA O ON (continued from previous page) EXHIBIT E.5 MRSA and Methicillin-Resistant Staphylococcus Aureus (or MRSA) Blood Infections C. Difficile Actual Expected Lower Upper Compare Cases Infections Cases CI Hospitals SIR CI to US Brigham and 5-997 0.916 3.282 Women's Hospital Tufts Medical 1 1.316 0.019 4.234 Center Brigham and 0.413 NA NA Women's Faulkner Hospital New England 0.222 NA Baptist Boston Medical 1 3.266 0.008 1.706 Center Beth Israel 1 4.083 0.006 1.365 Deaconess Medical Center Massachusetts 7.11 0.31 1.837 General Hospital Clostridium Difficile Infections Actual Expected Lower Upper Compare Hospitals Cases Cases SIR CI CI to US Brigham and 25 43.602 0.371 0.846 Women's Hospital Tufts Medical 14 21.001 0.364 1.119 Center Brigham and 0.113 1.605 Women's Faulkner Hospital New England 3 4.075 0.152 2.151 Baptist Boston Medical 37 21.704 2.35 Center Beth Israel 42 40.415 Deaconess Medical 0.749 1.405 Center 3 5.462 86 Massachusetts General Hospital 69.13 0.995 1.536 Source: Medicare.gov (2014b). [continued 574 Capstone Cases Cause Caus CAPSTONE CASE E: QUALITY OF CARE IN SEVEN BOSTON HOSPITALS wat is actually done to the patient, that is the sequence and coordi sation of activities. These include the technical aspects of care, or the scence of care activities of professionals well as the interper sonal spects of care or the art of caree, how patients are treated Process measures tend to be easier to collect the outcome measures Sess time dependent, and less dependent on peuve patient follow The medical record does track some but not all aspects of process of care. Process of care measures do depend on agreed upon criteria for care. Outcome measures refer to the changes in health status as a result of care. It is multidimensional and may include peal health status indicators as well as adverse outcomes of care such as Infections, complications, mortality and reasons. By Steven T. Reming The Affordable Care Acted a hospital value-based puh (VEP) program at the Centers for Medicare & Medical Services that rewards acute care hospitals with incentive payments for the y of care they provide to Medicare patients. The Hospital com program collects various structure, process, and outcome Indian for quality of care that are used by the VS gram. Thische compares seven Boston hospitals inters of these indicat Brigham and Women's Hospital is a bed teaching her associated with the Harvard Medical School atrak quality of medical care and has deep historical carly nineteenth century Brigham and Women's 3150-bed community teaching hospital founded in onda in southwest Boston Tufts Medical Center is 345-bed pital amiliated with Tufts School of Medicine and located Boston. New England Baptist hospitalisa-bed hospital with national reputation for the treatment of orthopedic and musculos etal conditions. Boston Medical Center is a 496-bed academic del center location in the South End neighborhood of Boston, Beth Deaconess Hospital is an 8-bed teaching hospital associated with the Harvard Medical School, Massachusetts General Hospital is the larg est and oldest hospital in New England. It is a so-bed medical center consistently ranked highly on the quality of care and reputation of the 16 clinical specialties Avedis Donabedian (1980) has proposed that quality of care be measured along three different dimensions: structure, process and outcome. Measures of structure relate to personnel, facilities and their configurations. Indicators such as fire code compliance, bacity cleanliness, physician licensure, and the ratio of RNs to total nurses would be considered measures of structure. This information is ready obtained from existing documents and inspection reports. One mar disadvantage of these measures is the assumption that the capacity to provide care structure) translates into the actual processes of which translates into favorable outcomes. Process measures refer to QUESTIONS 1. NE.slist seven structure measures for the seven Boston hospitals, which hospitals lack some measures that are presumably indicative of the capacity to provide care! 2. Bibit Lisa on haustive list of some process of care measures used by the VP. These measures we criteris deemed to be important for patient care. They document the percent of a sample of patients in which each measure is satisfied compared to Massachusetts and national averages. Why are these measures called process of care measures? 3. Compare Brigham and Women's Hospital to state and national Healthcare-associated infections are diverse outcomes of Care that are presumably associated with quality. These measures use a standardized infection ratio (SIR) to adjust for differences in the characteristics of patients using the hospital. They take into account type of patient care location, procedure, number of patients admitted with methicillin-resistant Staphylococcus (MRSA) or Cafe laboratory methods, hospital affiliation with a medical school, and bedste of the patient care location. The si is somewhat similar to the standardered mortality ratio (SMR) of the Indirect method of age adjusted mortality in that we calculate the expected number of infec. ons based on national benchmarks and adjustments. A confidence EXHIBIT E 1 Structure Measures Candia Bedstry Care Sora Debos Y Tufts Medical Center Y Y Y Y T Y Y Y 7. Y N Y Y Y Y Y Y Y N New England Bart Boston Medical Center Beth Deacon Medical N Y Y 1 Y Y Y Y Y Y Y Y Y y Y Y Y Y Y Y Y Y Y Y Note:?table data Source: Medicare gou Coul ant Mais EXHIBIT E.2 Timely and ffective Care Criteria (Not Exhaustive List) Tunts B&W NEB Best Bath Center Mortal Center 94 *** 94 + 0 100 Heart failure patients en discharge Heart failure patients gives an evaluation of left ventricular systoli VS) Action Heart failure patients given ACE ARB for left ventricular systolic dysfunction (SO) Pneumonia patients whose initial emergency room blood culture was performed prior to the administration of the hospital dose of ++ 99 94 95 AT 2 NA 95 * 95 37 Pneumonia patients given the most appropriate Initial antibiotic Outpatients having surgery who got an antibiotik at the right time with one hour before surgery Surgery in whose preventive antibiotics were stopped at the right time within 24 hours 99 100 99 Patients who got treatment at the right with 4 hours before or after the surgery to help prevent blood clots after certain types of 3 8 3 3 Surgery patients who were taking heart drugs called Bret Hackers before coming to the hospital, who were on the beachers during the periods before and after their Surgery patients who were given the right and of to help prevention Surgery patients whose nary catheters were removed on the Best or second day after surgery . 9 9 37 578 Capstone Cases Capstone Cases 529 18 82 Interval is estimated around the SIR and compared to the national SIR, which is to for each infection are. If the upper confidence limit is less than 1.0, the hospital is better than the national average because it had fewer Infections than expected. If the lower confidence it is greater than 1.0, then the hospital is worse than the nationale because it had more infections than expected. If the upper and lower confidence intervals include 1o, then the hospitals infection rate is the same neither better or worse) as the US average (Medicare. 2 2014). 8 3 16 QUESTIONS Exhibit E.3 summarizes central line and catheter associated infections for each hospital. Use Exhibit E.3 as a template to calculate the SIR for each hospital 5. Indikate whether each hospital is better worse, or the same as the United States average 6 2 2 & DDHIBITE.3 Central Line and Catheter Infections Put 16 Mass 98 90 Hospit Beth Mass Center B&W NE Baptist Boston Hospital NA MA Tufts 95 Brigha Ischemic stroke patients who received medicine known to prevent complications caused by blood cols within two days of anting at the hospital Hichem or hemorrhagle stroke received treatment to whe forming anywhere in the body within two doo Patients who got treatment to prevent blood com of or day her hospitali on the day of List) EXHIBIT 2 Timely and Effective Care Criteria (Not Exhaustive (continued) ker Hospital Medical General Ave arriving at the who Central Line-Associated Bloodstream Infections Actual Expected SIR Lower Upper Compare Hospitals Cases CI to US Brigham and 41.578 Women's Hospital 0.331 0.81 Tufts Medical 10 26.655 0.18 0.69 Center Brigham and 0 1.744 NA 2.135 Women's Faulkner Hospital New England 1 1.333 0.019 4.58 Baptist Boston Medical 3 24.067 0.06 0.364 Center Beth Israel 15 30.307 0.277 0.816 Deaconess Medical Sows MedicareGo Center Massachusetts General Hospital 38 66.796 0.403.7 EXHIBIT L3 Central Line and Catheter Infections (continued EXHIBIT LA Surgical Site Infections Actual Cases 89 pected SIR Lower User Compare . CI to US 21.733 0.491 1.309 18 7 3.719 0.757-88 3 2.66 Catheter Associated Urinary Tract Infections Actual Expected Sir Lower Upper Compa Hospitals Cases Cases CI Brigham and Women's Hospital 60.273 1.186 1.817 Tufts Medical 37 22.699 Center Brigham and 3-326 0.186 Women's Faulkner Hospital New England 1.641 0.148 Baptist 4403 Boston Medical 31 25.753 0.88 1709 Center Beth Israel 73 38.408 2.39 Deaconess Medical Center Massachusetts 200 86.373 2.006 2.66 General Hospital Brigham and Women's Hospital Tufts Medical Center Brigham and Women's Faulkner Hospital New England L53 2.443 N NA NA NA NA 2 5-58 0.043 1395 19 12.215 Boston Medical Center Beth Israel Deaconess Medical Center Massachusetts General Hospital 1.6 0:45 25 15-914 1.056 2.39 Source Medicare.gov Ch. Abdominal Hysterectomy Actual Expected SIR Lower Upper Compare a to US 5 4.895 0.332 2384 3 0.922 NA NA 6. Exhibit E4 summarizes surgical site infections for colon Surgery and abdominal hysterectomy for each hospital. Use Exhibit 425 a template to calculate the SiR for each hospital 7. Indicate whether each hospital is better, worse, or the same as the United States average. 8. Exhibit E.5 summarizes MRSA and C difficile for each hospital, Use Exhibit E.5 as a template to calculate the SIR for each hospital 9. Indicate whether each hospital is better, worse, or the same as the United States average. 0 0.419 NA NA Hospitals Brigham and Women's Hospital Tufts Medical Center Brigham and Women's Faulkner Hospital New England Baptist Boston Medical Center Beth Israel Deaconess Medical Center Massachusetts General Hospital NA NA NA NA 1.603 NA 2.301 2 2.616 The VBP also evaluates hospital 30-day mortality rates for acute myocardial infarction (AMI), congestive heart failure (CHF), and new monia. Confidence intervals are estimated for each hospital rate and compared to national norms. If the upper conlidence limit is less than US mortality rate, then the hospital is better than the national average if the lower confidence limit is greater than the US mortality rate, then 0.093 2.763 7 0.745.818 582 Capstone Cases 1 NA O ON (continued from previous page) EXHIBIT E.5 MRSA and Methicillin-Resistant Staphylococcus Aureus (or MRSA) Blood Infections C. Difficile Actual Expected Lower Upper Compare Cases Infections Cases CI Hospitals SIR CI to US Brigham and 5-997 0.916 3.282 Women's Hospital Tufts Medical 1 1.316 0.019 4.234 Center Brigham and 0.413 NA NA Women's Faulkner Hospital New England 0.222 NA Baptist Boston Medical 1 3.266 0.008 1.706 Center Beth Israel 1 4.083 0.006 1.365 Deaconess Medical Center Massachusetts 7.11 0.31 1.837 General Hospital Clostridium Difficile Infections Actual Expected Lower Upper Compare Hospitals Cases Cases SIR CI CI to US Brigham and 25 43.602 0.371 0.846 Women's Hospital Tufts Medical 14 21.001 0.364 1.119 Center Brigham and 0.113 1.605 Women's Faulkner Hospital New England 3 4.075 0.152 2.151 Baptist Boston Medical 37 21.704 2.35 Center Beth Israel 42 40.415 Deaconess Medical 0.749 1.405 Center 3 5.462 86 Massachusetts General Hospital 69.13 0.995 1.536 Source: Medicare.gov (2014b). [continued