As the team creates the CONOPS it will build a list of assumptions and constraints. Assumptions are circumstances and events that need to occur for the project to be successful, but are outside the total control of the project team. Assumptions are accepted as true and are often without proof or demonstration. Constraints are things that might restrict, limit, or regulate the project. Generally constraints are outside the total control of the project team.
Good luck on the project and let your instructor know if you have questions!
Unit 1 - Development of CONOPS Template:
Create a Concept of Operations (CONOPS) template for the surgery unit in the BCMH mini case (page 18 in textbook).
The CONOPS template needs to state the mission and goals of the BCMH surgical unit, along with the following: 1) defined operational objectives for the surgery unit; 2) assumptions, barriers, and constraints for operations management of the surgery unit based on the textbook scenario and additional information provided by the instructor; and 3) how the operational objectives will be measured.
Unit 2 - Concept of Operations Data Collection:
Add a data collection plan section to the CONOPS template created in Unit 1. The plan must include: 1) data items to be collected, and how they are used in operational management of BCMHs surgical unit; 2) the descriptive statistics required to analyze the data; and 3) a list of charts and graphs needed to brief leadership on operational effectiveness of the surgical unit. The team needs to justify why each chart and graph is required to measure operational effectiveness.
Assumptions, barriers, and constraints for your data collection plan need to be added to those already in the CONOPS.
Unit 3 - Concept of Operations, Decision Making:
Labor cost has gotten the attention of BMCH Leadership, and they want your team to come up with options addressing nurse staffing. The team must come up with at least three options for nurse staffing to include outsourcing 100% of the nurses, and formulate a decision-making framework for selecting the best option.
Assumptions, barriers, and constraints for your decision-making framework need to be added to those already in the CONOPS.
Unit 4 - Concept of Operations, Process Improvement and Risk Management:
Add a process improvement plan section to the CONOPS. The plan needs to address how the operational staff will review data and a process for continuous improvement. Risks to the surgical units operations need to be listed as well, along with how each risk will be mitigated.
Assumptions, barriers, and constraints for your risk management plan need to be added to those already in the CONOPS.
Lastly, the team will start preparation for a PowerPoint briefing that will be used to brief BMCH leadership on the final CONOPS. This briefing will be delivered in Unit 8 via the Big Blue Button in Canvas.
Unit 5 - Concept of Operations, Quality Improvement:
Add a quality improvement plan section to the CONOPS. The plan needs to list all quality metrics the team feels are important, to include patients, staff, and other stakeholders of BMCH. In addition, describe how each quality metric supports the operational objectives. Include a cost for implementing and measuring each quality metric.
Assumptions, barriers, and constraints for your quality improvement plan need to be added to those already in the CONOPS.
The Unit 8 briefing should be edited to include the quality improvement plan.
Unit 6 - Concept of Operations, Forecasting:
Add a forecasting plan section to the CONOPS for managing the surgery unit. The team needs to develop a physical layout for the unit, establish an operational day in hours, and estimate the number of surgical procedures needed to meet demand.
Assumptions, barriers, and constraints for your forecasting plan need to be added to those already in the CONOPS.
The forecasting plan needs to be added to the Unit 8 briefing.
Unit 7 - Concept of Operations, Scheduling and Capacity Planning:
Your team will present a PowerPoint presentation on the CONOPS to your professor, who roleplay the Chief of Staff at BCMH.
Add a scheduling and capacity management plan section to the CONOPS for managing the surgery unit. The team needs to develop a schedule for the surgery rooms, surgery staff, and disinfection/sterilization staff.
Assumptions, barriers, and constraints for your plan need to be clearly stated.
The scheduling and capacity management plan needs to be added to the Unit 8 briefing.
Team Project - Concept of Operations
Project Description: Teams will develop a Concept of Operations (CONOPS) for a health care organization. The CONOPS will be created in Units 1-7 and presented to the instructor using the Big Blue Button in Canvas during Unit 7.
The CONOPS creation starts with a template, which the team will create in Unit 1. This template will be updated and populated with content in Units 2-7. There is not a standard template for a CONOPS, rather it depends on the organizations mission and operating environment. The team may come up with its own CONOPS template, and it will be updated as the CONOPS is created. The team will be graded on the final CONOPS submitted in Unit 8, so interim draft copies starting with the template can be modified as needed to achieve the final version.
A CONOPS states how operations will be conducted by an organization, and provides guidance to the staff for various aspects of operations. As mentioned above, a CONOPS depends on the organizations mission and operating environment. For example, take two walk-in urgent care clinics, one located in a large urban hospital and the other in a rural area where the closest hospital is miles away. Both have the same mission, i.e. to provide urgent care health care services, but their operating environments are much different. For the urgent care clinic inside the urban hospital it is possible to for the clinic staff to obtain hospital resources, utilize hospital staff, and transfer critical patients to the ER, surgery, etc. Whereas the clinic in the rural environment needs staff to be prepared to stabilize and transport patients a greater distance and they must have everything needed on site.
The following example CONOPS is provided so teams can get some idea of what a CONOPS looks like.
CONOPS Example
Of course, the CONOPS for the HA612 team project will not be as large as the example. However, it needs to contain the content described below for Units 1 7 and the team has freedom to define operations as they see fit. In other words, there is no set CONOPS for the project, rather the team will define the CONOPS from their understanding of the organizations mission, goals, and objectives. No two teams will end up with the same CONOPS. The CONOPS needs to have a separate section for each item required in Units 2-7.
As the team creates the CONOPS it will build a list of assumptions and constraints. Assumptions are circumstances and events that need to occur for the project to be successful, but are outside the total control of the project team. Assumptions are accepted as true and are often without proof or demonstration. Constraints are things that might restrict, limit, or regulate the project. Generally constraints are outside the total control of the project team.
Good luck on the project and let your instructor know if you have questions!
Unit 1 - Development of CONOPS Template:
Create a Concept of Operations (CONOPS) template for the surgery unit in the BCMH mini case (page 18 in textbook).
The CONOPS template needs to state the mission and goals of the BCMH surgical unit, along with the following: 1) defined operational objectives for the surgery unit; 2) assumptions, barriers, and constraints for operations management of the surgery unit based on the textbook scenario and additional information provided by the instructor; and 3) how the operational objectives will be measured.
Unit 2 - Concept of Operations Data Collection:
Add a data collection plan section to the CONOPS template created in Unit 1. The plan must include: 1) data items to be collected, and how they are used in operational management of BCMHs surgical unit; 2) the descriptive statistics required to analyze the data; and 3) a list of charts and graphs needed to brief leadership on operational effectiveness of the surgical unit. The team needs to justify why each chart and graph is required to measure operational effectiveness.
Assumptions, barriers, and constraints for your data collection plan need to be added to those already in the CONOPS.
Unit 3 - Concept of Operations, Decision Making:
Labor cost has gotten the attention of BMCH Leadership, and they want your team to come up with options addressing nurse staffing. The team must come up with at least three options for nurse staffing to include outsourcing 100% of the nurses, and formulate a decision-making framework for selecting the best option.
Assumptions, barriers, and constraints for your decision-making framework need to be added to those already in the CONOPS.
Unit 4 - Concept of Operations, Process Improvement and Risk Management:
Add a process improvement plan section to the CONOPS. The plan needs to address how the operational staff will review data and a process for continuous improvement. Risks to the surgical units operations need to be listed as well, along with how each risk will be mitigated.
Assumptions, barriers, and constraints for your risk management plan need to be added to those already in the CONOPS.
Lastly, the team will start preparation for a PowerPoint briefing that will be used to brief BMCH leadership on the final CONOPS. This briefing will be delivered in Unit 8 via the Big Blue Button in Canvas.
Unit 5 - Concept of Operations, Quality Improvement:
Add a quality improvement plan section to the CONOPS. The plan needs to list all quality metrics the team feels are important, to include patients, staff, and other stakeholders of BMCH. In addition, describe how each quality metric supports the operational objectives. Include a cost for implementing and measuring each quality metric.
Assumptions, barriers, and constraints for your quality improvement plan need to be added to those already in the CONOPS.
The Unit 8 briefing should be edited to include the quality improvement plan.
Unit 6 - Concept of Operations, Forecasting:
Add a forecasting plan section to the CONOPS for managing the surgery unit. The team needs to develop a physical layout for the unit, establish an operational day in hours, and estimate the number of surgical procedures needed to meet demand.
Assumptions, barriers, and constraints for your forecasting plan need to be added to those already in the CONOPS.
The forecasting plan needs to be added to the Unit 8 briefing.
Unit 7 - Concept of Operations, Scheduling and Capacity Planning:
Your team will present a PowerPoint presentation on the CONOPS to your professor, who roleplay the Chief of Staff at BCMH.
Presentation length is 20-30 minutes, and the quality of slides should be appropriate for briefing a senior leader.
The presentation needs to be equally divided amongst the team members.
Team should prepare for a 5-10 minute question period at the end of their presentation.
Note: avoid using videos and sound in the presentation because they will not work on the Big Blue Button in Canvas.
Add a scheduling and capacity management plan section to the CONOPS for managing the surgery unit. The team needs to develop a schedule for the surgery rooms, surgery staff, and disinfection/sterilization staff.
Assumptions, barriers, and constraints for your plan need to be clearly stated.
The scheduling and capacity management plan needs to be added to the Unit 8 briefing.
Unit 8 - CONOPS Deliverable:
The team will submit the CONOPS document.
Team Project Guidelines
Team Formation (0 points)
The instructor will assemble project work teams, which will consist of a Project Manager (PM) and team members. The assigned PM will be the team leader and will be responsible for planning, organizing, directing, controlling, and coordinating the effort of the team to ensure that the assigned project and its deliverables are successfully completed by the established deadline. Team sizes may vary based on courses enrollment and the nature and scope of the projects to be completed; however, the total team will have no fewer than three (3) and no more than four (4). The goal is to keep the team sizes small enough that each member will have an equal opportunity to make a substantive contribution to the overall success of the team in terms of meeting its goals and objectives.
Important Notice: It is at the sole discretion of the instructor to change team members with or without advance notice for cause or for no reason at all. In addition, the instructor has the right to change the parameters of the team projects, including, but not limited to: moving up or pushing back due dates, changing deliverable expectations, or request progress reports.
Team Meetings - Units 2-7 (0 points Units 2-6, 42 points Unit 7)
Online Students: Each team will utilize Zoom to conduct and record their team meeting. Failure to record any of these mandatory meetings will adversely affect the both PM and team members grade, which will be assigned by the faculty at the end of unit 7. The meeting MUST be conducted at some point during the unit, which runs from Monday through Sunday. This will allow ample flexibility to accommodate work schedules and the geographic location of the participants (domestic or international). It is expected that a typical meeting will last 45 minutes to an hour depending on the level of group and individual preparation; however, there is no artificial limitations on the length of time the team can participate in the meeting. Zoom facilitates the sharing of ones computer screen, which makes it possible to use these meetings as actual work session. There is no long distance charge associated with using Zoom.
Blended Students: There will be dedicated time during each class session for each team to meet. The time allotted to this activity may vary based on the lesson plan. It IS NOT expected that these in-class meetings will be adequate to ensure the successful completion of the assignment project. In fact, it is more likely that additional meetings outside of class will be required. Assuming this is the case, each team will be permitted to meet using Zoom. These out-of-class meetings WILL NOT need to be recorded; however, they may be recorded should the PM find this helpful. Zoom facilitates the sharing of ones computer screen, which makes it possible to use these meetings as actual work session. There is no long distance charge associated with using Zoom.
Team participants are responsible for viewing the tutorials on how to access and function within Zoom. See Using Zoom: Students.
Team Project Descriptions
Team Project: Concept of Operations (CONOPS)
Unit Learning Outcomes:
Unit 1:
ULO #1: Formulate operational objectives for a health care organization that support the organizations mission statement and strategic objectives. (CLO 1, 2, 3, 4, 5, 6, and 7)
ULO #2: Prepare a template for a concept of operations whose goal is to achieve the operational objectives in ULO #1. (CLO 1, 2, 3, 4, 5, 6, and 7)
ULO #3: Formulate the measurement criteria needed determine when operational objectives in ULO #1 are achieved.
Unit 2:
ULO #2: Formulate a data collection plan to measure effectiveness of an organizations operations. (CLO 3, 4, and 5)
ULO #3: Formulate recommendations to strategic managers for optimizing operational effectiveness using data. (CLO 1, 3, 4, 5, and 7)
Unit 3:
ULO #1: Determine the barriers, constraints, and problems the operational manager is likely to encounter in a health care organization. (CLO 2, 3, 4, and 5)
ULO #2: Design strategies intended to garner personnel support for the concept of operations. (CLO 1, 3, 4, 5, 6, and 7)
ULO #3: Analyze data and formulate a decision-making process for selecting potential courses of action. (CLO 2, 3, 4, and 5)
Unit 4:
ULO #1: Prepare a process improvement plan for a health care organization. (CLO 2, 4, 5, 6, and 7)
ULO #2: Identify risks to a health care organization resulting from a poorly designed process flow. (CLO 2, 6, and 7)
ULO #3: Identify considerations for optimizing facility layout of a health care organization. (CLO 2, 6, and 7)
Unit 5:
ULO #1: Formulate a plan to manage quality in a health care organizations products and services, and incorporate quality improvement. (CLO 2, 3, 4, 5, 6 and 7)
ULO #3: Identify whether quality management metrics are adequate to protect the healthcare organization. (CLO 1, 4 and 7)Unit 6:
Unit 6:
ULO #1: Develop a plan for forecasting impacts to a healthcare organizations bottom line if an industry changing event occurs, e.g. passage of Affordable Care Act. (CLO 1, 2, 4, and 7)
Unit 7:
ULO #2: Evaluate the capacity of a health care organization based on forecasting and adjust planning, scheduling and capacity management to accommodate the forecast. (CLO 3, 4, 5, 6, and 7)
ULO #3: Asses the risk to the organization if forecast is incorrect, brief senior management, and update risk plan in concept of operations. (CLO 4, 5, 6, and 7)Unit 8:
Unit 8:
ULO #1: Develop a concept of operations and present it to senior managers. (CLO 1, 2, 3, 4, 5, 6 and 7)
ULO #2: Formulate a data collection plan to support concept of operations and measure operations performance. (CLO 3, 4, 5 and 6)
ULO #3: Identify potential barriers, constraints, and problems operations managers may encounter, and develop mitigation plans for dealing with each. (CLO 2, 3, 4 and 5)
ULO #4: Evaluate risks to operations and develop risk management plan. (CLO 4, 5, 6 and 7)
ULO #5: Design and execute a project plan for implementing a concept of operations. (CLO 6)
ULO #6: Evaluate current capacity using data and information systems, then create a plan for modifying capacity and scheduling. (CLO 3, 4, 5, and 7)
Introduction to Team Project:
According to the U.S. Department of Transportation Federal Highway Administration, the Concept of Operations is a description of how a system will be used. It is non-technical, and presented from the viewpoints of the various stakeholders. This provides a bridge between the often vague needs that motivated the project to begin with and the specific technical requirements. There are several reasons for developing a Concept of Operations .
Get stakeholder agreement identifying how the system is to be operated, who is responsible for what, and what the lines of communication are
Define the high-level system concept and justify that it is superior to the other alternatives
Define the environment in which the system will operate
Derive high-level requirements, especially user requirements
Provide the criteria to be used for validation of the completed system
There are number of methodologies used in the construction of a Concept of Operations. According to Carnegie Mellon University (2008), there are some commonalities associated with the development of a CONOPS and they are:
Statement of the goals and objectives of the system
Strategies, tactics,policies , and constraints affecting the system
Organizations, activities, and interactions among participants and stakeholders
Clear statement of responsibilities and authorities delegated
Specific operational processes for fielding the system
Processes for initiating, developing, maintaining, and retiring the system
It is envisioned that the development of a CONOPS provider a clear methodology to realize the goals and objectives for the system, but is not expected to be used as an implementation or transition plan itself.
Sources:
Concepts of Operations. Carnegie Mellon University 2008.
IEEE Std. 1362-1998 IEEE Guide for Information TechnologySystem DefinitionConcept of Operations (ConOps) Document. IEEE Standards Association.
IEEE Std. 29148-2011 Systems and Software EngineeringLife Cycle ProcessesRequirements Engineering
Directions
The team will create a Concept of Operations (CONOPS) for the Operating Room Department depicted in the mini-case: The Bullwhip Effect in Health Care Organizations, which can be found on pages 18 and 19 of the textbook. The CONOPS needs to address, but is not limited to the following:
Statement of the goals and objectives of the system
Strategies, tactics,policies , and constraints affecting the system
Organizations, activities, and interactions among participants and stakeholders
Clear statement of responsibilities and authorities delegated
Specific operational processes for fielding the system
Processes for initiating, developing, maintaining, and retiring the system
It is understood that the mini-case, that is the focus on this team project, wasnt designed specifically to support the creation of a CONOPS, so you will be expected to create additional information to augment the case. The additional information used to complete the project MUST be realistic and reflect the teams effort to research comparable OR Departments.
Important Notice: It is at the sole discretion of the instructor to change team members with or without advance notice for cause or for no reason at all. In addition, the instructor has the right to change the parameters of the team projects, including, but not limited to: moving up or pushing back due dates, changing deliverable expectations, or request progress reports.
Team Project Deliverable Description (160 points)
There are NO page limits associated with this deliverable; however, it is expected the quality of the product will be consistent with that expected of an industry professional. Special attention should be given to the quality and accuracy of the content; the layout of the content; and ensuring the topics flow logically throughout the document. The teams SHOIULD NOT use a question & answer format. The submission must adhere to the APA writing style (6th edition). Use Microsoft Excel spreadsheets to perform financial calculations. The Team Project Deliverable should be prepared as a Microsoft Word document and uploaded in the appropriate Unit 8 assignment page by Friday, 11:59 p.m. (CT).
PowerPoint and Oral Presentation Description (62 points)
There is NO prescribed number of slides that must be contained within the slide deck. Specific criteria for the successful completion of the presentation (slides and oral delivery) are clearly laid out within the Presentation Grading Rubric. All participants are expected to dress in acceptable business attire and actively present content to the audience.
Blended students will deliver their presentation in the classroom before a live audience during the seventh week of the term. Online students will deliver and record their presentation using Zoom before a live, remote audience. The PM will need to ascertain a date and time that will maximize audience participation. The recording of the presentation is to be submitted by Sunday, at 11:59 p.m. (CT).
For both the blended and online students, the PowerPoint slides are due by Sunday, at 11:59 p.m. (CT), and are to be uploaded under the appropriate Unit 7 assignment page. The PM is responsible for ensuring the slides are correctly uploaded by the deadline
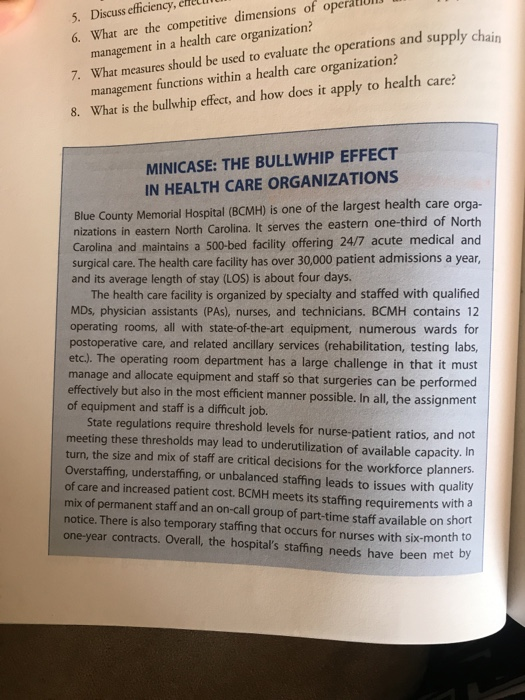
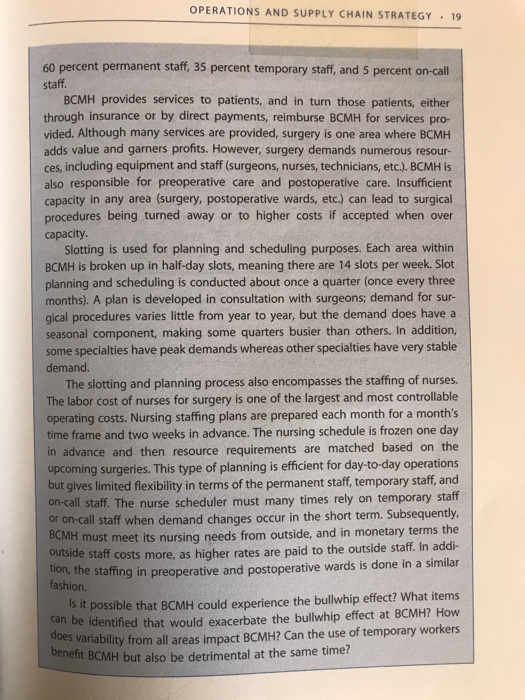
5. Discuss efficiency, 6. What are the competitive dimensions of ope management in a health care organization? 7. What measures should be used to evaluate the operations and supply chain management functions within a health care organization? 8. What is the bullwhip effect, and how does it apply to health care? MINICASE: THE BULLWHIP EFFECT IN HEALTH CARE ORGANIZATIONS Blue County Memorial Hospital (BCMH) is one of the largest health care orga- nizations in easte North Carolina. It serves the eastern one-third of North Carolina and maintains a 500-bed facility offering 24/7 acute medical and surgical care. The health care facility has over 30,000 patient admissions a year, and its average length of stay (LOS) is about four days. The health care facility is organized by specialty and staffed with qualified MDs, physician assistants (PAs), nurses, and technicians. BCMH contains 12 operating rooms, all with state-of-the-art equipment, numerous wards for postoperative care, and related ancillary services (rehabilitation, testing labs, etc.). The operating room department has a large challenge in that it must manage and allocate equipment and staff so that surgeries can be performed effectively but also in the most efficient manner possible. In all, the assignment of equipment and staff is a difficult job. State regulations require threshold levels for nurse-patient ratios, and not meeting these thresholds may lead to underutilization of available capacity. In turn, the size and mix of staff are critical decisions for the workforce planners. Overstaffing, understaffing, or unbalanced staffing leads to issues with quality of care and increased patient cost. BCMH meets its staffing requirements with a mix of permanent staff and an on-call group of part-time staff available on short notice. There is also temporary staffing that occurs for nurses with six-month to one-year contracts. Overall, the hospital's staffing needs have been met by benefit BCMH but also be detrimental at the same time? OPERATIONS AND SUPPLY CHAIN STRATEGY 19 60 percent permanent staff, 35 percent temporary staff, and 5 percent on-call staff. BCMH provides services to patients, and in turn those patients, either through insurance or by direct payments, reimburse BCMH for services pro- vided. Although many services are provided, surgery is one area where BCMH adds value and garners profits. However, surgery demands numerous resour- ces, including equipment and staff (surgeons, nurses, technicians, etc.). BCMH is also responsible for preoperative care and postoperative care. Insufficient capacity in any area (surgery, postoperative wards, etc.) can lead to surgical procedures being turned away or to higher costs if accepted when over capacity. Slotting is used for planning and scheduling purposes. Each area within BCMH is broken up in half-day slots, meaning there are 14 slots per week. Slot planning and scheduling is conducted about once a quarter (once every three months). A plan is developed in consultation with surgeons; demand for sur- gical procedures varies little from year to year, but the demand does have a seasonal component, making some quarters busier than others. In addition, some specialties have peak demands whereas other specialties have very stable demand. The slotting and planning process also encompasses the staffing of nurses. The labor cost of nurses for surgery is one of the largest and most controllable operating costs. Nursing staffing plans are prepared each month for a month's time frame and two weeks in advance. The nursing schedule is frozen one day in advance and then resource requirements are matched based on the upcoming surgeries. This type of planning is efficient for day-to-day operations but gives limited flexibility in terms of the permanent staff, temporary staff, and on-call staff. The nurse scheduler must many times rely on temporary staff or on-call staff when demand changes occur in the short term. Subsequently, BCMH must meet its nursing needs from outside, and in monetary terms the outside staff costs more, as higher rates are paid to the outside staff. In addi- tion, the staffing in preoperative and postoperative wards is done in a similar Is it possible that BCMH could experience the bullwhip effect? What items can be identified that would exacerbate the bullwhip effect at BCMH? How does variability from all areas impact BCMH? Can the use of temporary workers fashion. 5. Discuss efficiency, 6. What are the competitive dimensions of ope management in a health care organization? 7. What measures should be used to evaluate the operations and supply chain management functions within a health care organization? 8. What is the bullwhip effect, and how does it apply to health care? MINICASE: THE BULLWHIP EFFECT IN HEALTH CARE ORGANIZATIONS Blue County Memorial Hospital (BCMH) is one of the largest health care orga- nizations in easte North Carolina. It serves the eastern one-third of North Carolina and maintains a 500-bed facility offering 24/7 acute medical and surgical care. The health care facility has over 30,000 patient admissions a year, and its average length of stay (LOS) is about four days. The health care facility is organized by specialty and staffed with qualified MDs, physician assistants (PAs), nurses, and technicians. BCMH contains 12 operating rooms, all with state-of-the-art equipment, numerous wards for postoperative care, and related ancillary services (rehabilitation, testing labs, etc.). The operating room department has a large challenge in that it must manage and allocate equipment and staff so that surgeries can be performed effectively but also in the most efficient manner possible. In all, the assignment of equipment and staff is a difficult job. State regulations require threshold levels for nurse-patient ratios, and not meeting these thresholds may lead to underutilization of available capacity. In turn, the size and mix of staff are critical decisions for the workforce planners. Overstaffing, understaffing, or unbalanced staffing leads to issues with quality of care and increased patient cost. BCMH meets its staffing requirements with a mix of permanent staff and an on-call group of part-time staff available on short notice. There is also temporary staffing that occurs for nurses with six-month to one-year contracts. Overall, the hospital's staffing needs have been met by benefit BCMH but also be detrimental at the same time? OPERATIONS AND SUPPLY CHAIN STRATEGY 19 60 percent permanent staff, 35 percent temporary staff, and 5 percent on-call staff. BCMH provides services to patients, and in turn those patients, either through insurance or by direct payments, reimburse BCMH for services pro- vided. Although many services are provided, surgery is one area where BCMH adds value and garners profits. However, surgery demands numerous resour- ces, including equipment and staff (surgeons, nurses, technicians, etc.). BCMH is also responsible for preoperative care and postoperative care. Insufficient capacity in any area (surgery, postoperative wards, etc.) can lead to surgical procedures being turned away or to higher costs if accepted when over capacity. Slotting is used for planning and scheduling purposes. Each area within BCMH is broken up in half-day slots, meaning there are 14 slots per week. Slot planning and scheduling is conducted about once a quarter (once every three months). A plan is developed in consultation with surgeons; demand for sur- gical procedures varies little from year to year, but the demand does have a seasonal component, making some quarters busier than others. In addition, some specialties have peak demands whereas other specialties have very stable demand. The slotting and planning process also encompasses the staffing of nurses. The labor cost of nurses for surgery is one of the largest and most controllable operating costs. Nursing staffing plans are prepared each month for a month's time frame and two weeks in advance. The nursing schedule is frozen one day in advance and then resource requirements are matched based on the upcoming surgeries. This type of planning is efficient for day-to-day operations but gives limited flexibility in terms of the permanent staff, temporary staff, and on-call staff. The nurse scheduler must many times rely on temporary staff or on-call staff when demand changes occur in the short term. Subsequently, BCMH must meet its nursing needs from outside, and in monetary terms the outside staff costs more, as higher rates are paid to the outside staff. In addi- tion, the staffing in preoperative and postoperative wards is done in a similar Is it possible that BCMH could experience the bullwhip effect? What items can be identified that would exacerbate the bullwhip effect at BCMH? How does variability from all areas impact BCMH? Can the use of temporary workers fashion