

Question: Case 11.2 Fighting AIDS in Asia (API), an NGO based in Washington, D.C., dedicated to slowing an active volunteer as an MBASAS API had been
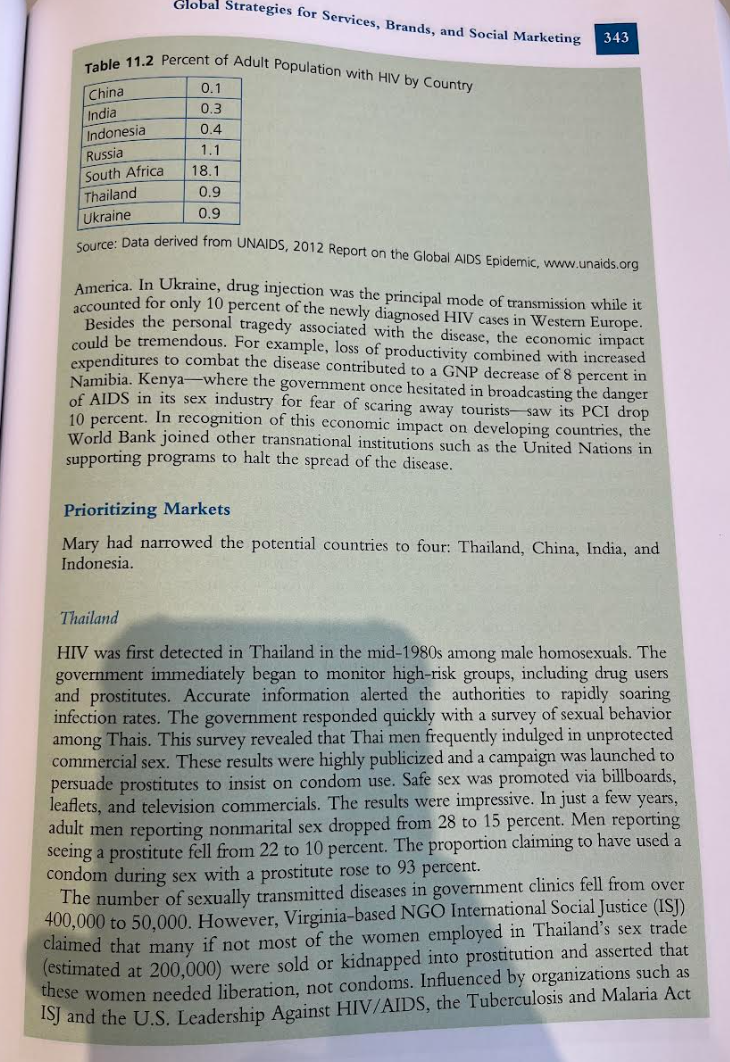
Case 11.2 Fighting AIDS in Asia (API), an NGO based in Washington, D.C., dedicated to slowing an active volunteer as an MBASAS API had been recently established by a very generous U.S. philanthropist. The investment return of API's current endowment would cover annual expenses for operating a headquarters located in the United States as well as small offices in up to four developing countries. In addition, funds would remain to support modert educational programs in these countries as well as further fundraising efforts. Mary believed that the NGO's resources could best be deployed by focusing on a few countries in Asia. She was currently in the process of prioritizing tatget countries and deciding which population segments within those countries to target. Other key questions involved the extent to which API should ally with local NGOs and governments and whether API should apply for funding from the U.S. government. The Global AIDS Epidemic HIV was first identified in the 1970s. (HIV is the virus that triggers AIDS.) The disease spread first among homosexuals, intravenous drug users, and workers in the sex industry but inevitably entered the general population. AIDS is now the world's fourth largest infectious killer. The disease first appeared in West Africa. After remaining relatively contained in the Congo's sparsely populated jungles, it began to spread rapidly via rebel armies and truck drivers who frequented brothels. AIDS was already devastating the African continent when it first ppeared in the United States in the early 1980s. Africa still remains the hardest iit area of the world. There were substantial differences in HIV prevalence rates by region. Intraregional ifferences at the country level could be substantial as well (see Table 11.2). The ighest estimates for new HIV/AIDS infections were in sub-Saharan Africa, Eastern urope, Central Asia, South Asia and Southeast Asia. Who was most at risk also ried by region. In Eastern Europe and Russia, most HIV-positive people wer der 30 years of age compared with only 30 percent in Western Europe and Nort Global Strategies for Services, Brands, and Social Marketing 343 Table 11.2 Percent of Adult Population with HIV by Country Source: Data derived from UNAIDS, 2012 Report on the Global AIDS Epidemic, uww.unaids.org America. In Ukraine, drug injection was the principal mode of transmission while it accounted for only 10 percent of the newly diagnosed HIV cases in Western Europe. Besides the personal tragedy associated with the disease, the economic impact could be tremendous. For example, loss of productivity combined with increased expenditures to combat the disease contributed to a GNP decrease of 8 percent in Namibia. Kenya-where the government once hesitated in broadcasting the danger of AIDS in its sex industry for fear of scaring away tourists- saw its PCI drop 10 percent. In recognition of this economic impact on developing countries, the World Bank joined other transnational institutions such as the United Nations in supporting programs to halt the spread of the disease. Prioritizing Markets Mary had narrowed the potential countries to four: Thailand, China, India, and Indonesia. Thailand HIV was first detected in Thailand in the mid-1980s among male homosexuals. The government immediately began to monitor high-risk groups, including drug users and prostitutes. Accurate information alerted the authorities to rapidly soaring infection rates. The government responded quickly with a survey of sexual behavior among Thais. This survey revealed that Thai men frequently indulged in unprotected commercial sex. These results were highly publicized and a campaign was launched to persuade prostitutes to insist on condom use. Safe sex was promoted via billboards, leaflets, and television commercials. The results were impressive. In just a few years, adult men reporting nonmarital sex dropped from 28 to 15 percent. Men reporting seeing a prostitute fell from 22 to 10 percent. The proportion claiming to have used a condom during sex with a prostitute rose to 93 percent. The number of sexually transmitted diseases in government clinics fell from over 400,000 to 50,000 . However, Virginia-based NGO International Social Justice (ISJ) claimed that many if not most of the women employed in Thailand's sex trade (estimated at 200,000) were sold or kidnapped into prostitution and asserted that these women needed liberation, not condoms. Influenced by organizations such as ISJ and the U.S. Leadership Against HIV/AIDS, the Tuberculosis and Malaria Act 344 Designing Global or did not have a policy explicilly Asian financial crisis, Thailand cut its expenthith of the Astenditures were still only about half of Furthermore, in the wake of for AIDS prevention. Years later, expenditures aigh armong drug users and gay men, m, l oh services such as needie exchange pron youth. Because earlier campaigns had asso become stigmatized. Condom by young men with steady girlfiends was low, and Local NGOs were calling for improved of pe parthers was on the rise among Thai teens. expanded sex education in Thai schools. Chind HIV first entered China in the late 1980 s via infected drug users. In the 1990s, a major epidemic arose in the province of Henan when villagers were recruited, to donate blood. In order to donate up to plasma had been extracted. Activists estimate that on with their own blood atter the plaion became infected with HIV. In one village alone, one-third of the addaht million became infected with contracted the disease. No one was ever held accountable. In fact, Ching? communist government was at first less than enthusiastic about raising AIDJ awareness, and many AIDS prevention volunteers reported being harassed by government authorities. Statistics concerning the disease were treated as a state secte, The government atrributed most AIDS cases to intravenous drug use. However, international agencies estimated that only about 60 percent of Chinese citizens infected with HIV/AIDS contracted the disease through the use of illicit drigs. Infection from unprotected sex was rising. China's younger generation was reaching puberty earlier and marrying later. Consequently, premarital sex was on the rise. Hundreds of millions of Chinese people were on the move as well, as the rural Chinese population poured into urban areas in search of jobs. Many of these migrants were males who left wives behind in the country. However, man migrants were women in search of jobs that often failed to materialize. The result was a booming commercial sex industry in Chinese cities. The govermment announced that it would redouble efforts to educate studens regarding AIDS and launched AIDS prevention websites aimed at youth. Despite the new push by the central government, many believed provincial goverments were ignoring-even covering up-the problem, and a surprising number of Chinese people remained unaware of the disease. Only years later did the Chines? government announce that AIDS prevention would be added to the country's educational curriculum. dia, with an estimated 2.4 million infected with HIV, ranked third after Soutt frica and Nigeria for the highest number of infected persons. In recognition of the government organized a Parliamentrons As in many developing countries, controversy surrounded AIDS statistics collected by the government. To address this problem, the Indian government hired a prestigious (and independent) private company to estimate the level of HIV/AIDS in India. reaching about 30 percent of the population. What prevention programs were only husbands were often blamed by their in-laws. NGOs who were infected by their patients or AIDS orphans were often evicted if their landlords discovered the nature of their operations. Police were even known to harass health workers who were Health workers in India believed that own AIDS prevention information. areas where prevention programs were the weakest was spreading fastest in rural Hope Foundation was disseminating AIDS inforest and record-keeping the worst. India's five million truckers covered 5,000 miles otion and condoms at truck stops. five sexual partners a week. In six years, the HIV infection rate among truckers fell from 10 to 4 percent. To address the threat of AIDS to young people, the government had established two national prizes to award colleges or youth groups who acted as agents of change by implementing their own AIDS awareness initiatives. Still AIDS carried a social declared that India's moral character and cored the country, many Indian officials the spread of AIDS. Sex was rarely a conservative sexual mores would prevent absent from Indian films, and schools offered litll public discourse. It was largely Nonetheless, numerous NGOs operated itle or no sex education. support for persons with HIV, general awat in India. Their programs included care for orphans whose parents died fromareness and educational programs, and state governments, international from AIDS. Funding came from federal and One international donor, donors, and local contributions. million for a ten-year prog, The Bill \& Melinda Gates Foundation, pledged $100 into the program, the Foun for AIDS prevention in India. However, several years profit organizations to the Indian government to run. The government was to air-coosic, noting that the costs of the network were astronomical. They pointed ditioned clinics and glossy English posters and brochures that the clinics' clentele could not read. In addition, top managers were paid salaries nsurate with MBA salaries in the West. Results were disappointing as well. Despite an expensive campaign aimed at truckers, an internal report concluded that only 12 percent of truckers were even aware of the program's services and only 7 percent ever used them. indonesia ndonesia historically enjoyed a low rate of HIV infection, but that was changing ist, particularly among drug users and throughout the nation's expandin ommercial sex industry where only one man in ten used a condom. The WHC d given Indonesia an even higher priority for AIDS attention than China hailand, and international AIDS prevention groups stated that the Indonesia vernment vastly under-reported the cases in the country. However, Indonesia was Islam's most populous country, and AIDS preventic deavors were proving controversial with conservative Muslims. Islam forba ramarital sex. One Muslim politician remarked that AIDS prevention shou focus on improving people's morality and not urge them to protect themsel t by by using condoms. The Indonesian Ulemas' Council, the country's highest authority, proclaimed that Muslims should fight AIDS by being more religiols ing closer to family. DKT Indonesia, a Washington-based NGO, produced a line of condoms the sold at discount rates in Indonesia to truck divers with Indonesia's MTV affiliate, hhe NGO also placed a few condom adver than images of real people. Attempts to th used dancing strawberry cartoons rather that other AIDS prevention advertisements aired were met with less success. A U.S.-based NGO. Family Health International, briefly aired a commercial thated depicted men visiting prostitutes. But fundamentalist Muslim clerics complained. The Indonesian government officially proposed new education programs in schoolis along with better training for health-care workers and voluntary Hiv testing and counseling. However, some within the goveducation and health care. Also, much of the country's health-care budget fell under the auspices of provincial governmenths sympathetic to views of Islamic fundamentalist groups. As one local AIDS activis noted: many considered AIDS a punishment from God for wrongdoing. Other viewed it as a Western phenomenon and nothing to do with them. As Mary contemplated the challenges of each of these four potential Asizan markets, she wondered whether any of her experience as a global product managet could be put to use in this new context of international social marketing. Discussion Questions 1. Given that there are many multinational and local "competitors" participating in the social marketing of AIDS prevention, what role should API play? What products/services could it deliver? 2. What elements of these services might be standardized across developing countries? What elements might need to be adapted? Why? 3. What suggestions would you give Mary for prioritizing the four Asian market?? 4. Should API partner with local governments? Local NGOs? Should it pursue funding from the U.S. government? 5. How might Mary's experience as a global product manager be useful in this new setting? Sources: "Fighting AIDS in Asia," in Kate Gillespie and H. David Hennessey, Glood Marketing (Mason, OH: Cengage, 2011), pp. 336-339; UNAIDS, World AIDS Day Report 2012; "HIV-AIDS Biggest Health Risk in Thailand," Australia Network Nens, August 21, 2013; Kate Kelland, "AIDS Proves Stubborn in Europe as New HIV Infections Rise," Reuters, November 27, 2013; "HIV/AIDS in India," World Bank News, July 10, 2012; Donald G. McNeil, Jr., "HIV Tests Urged for 800 Milliion in India," New York: Times, June 17, 2013; Tan Ee Lyn and Fitri Wulandari, "With Head in Sand, Indonsis itruggles to Tackle AIDS," Reuters, April 12, 2011; and "China: In Need of Mort rotection," The Economist, January 30,2014
Step by Step Solution
There are 3 Steps involved in it

Get step-by-step solutions from verified subject matter experts