

Question: Chapter 6 Chapter 6 Chapter 7 Chapter 8 Help me, please Please explain Answers in details Controlling and Allocating Resources 575 CHAPTER 11 Case Study
Chapter 6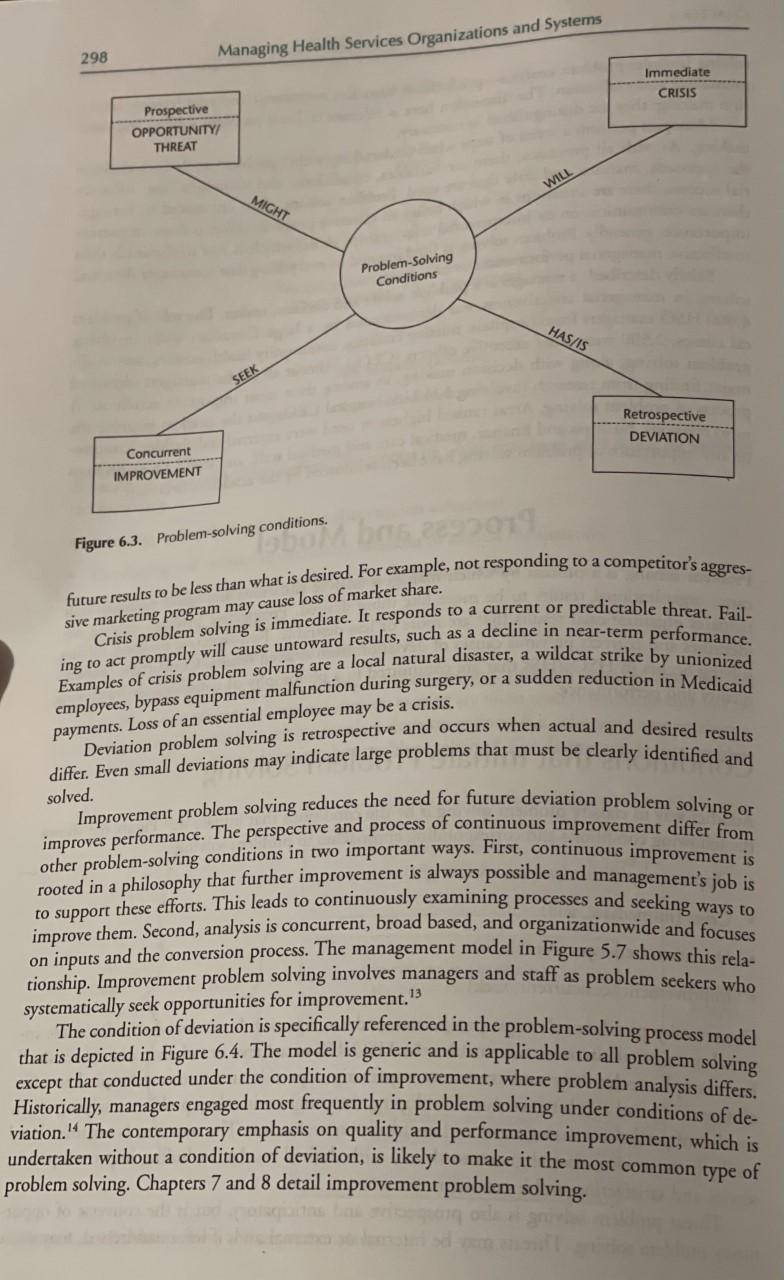
Chapter 6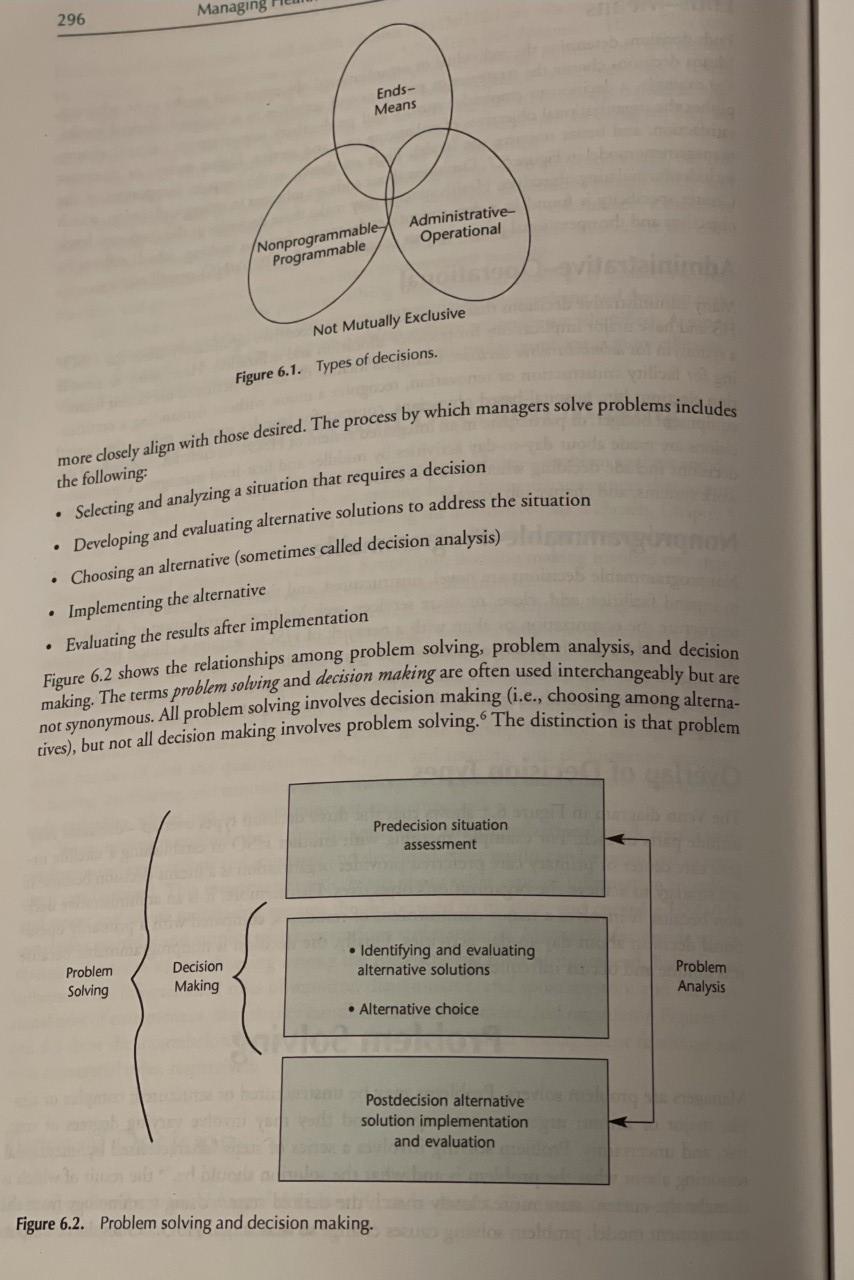
Chapter 7 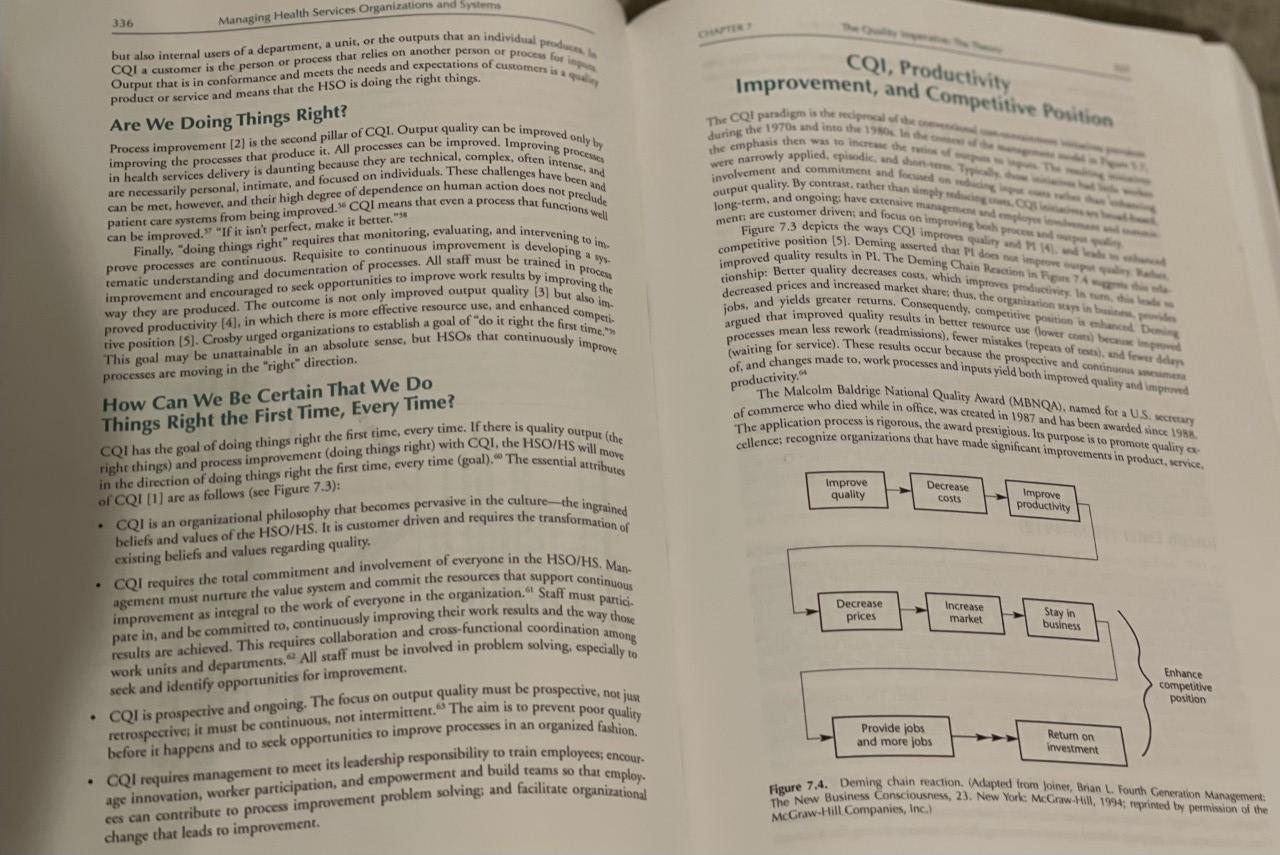
Chapter 8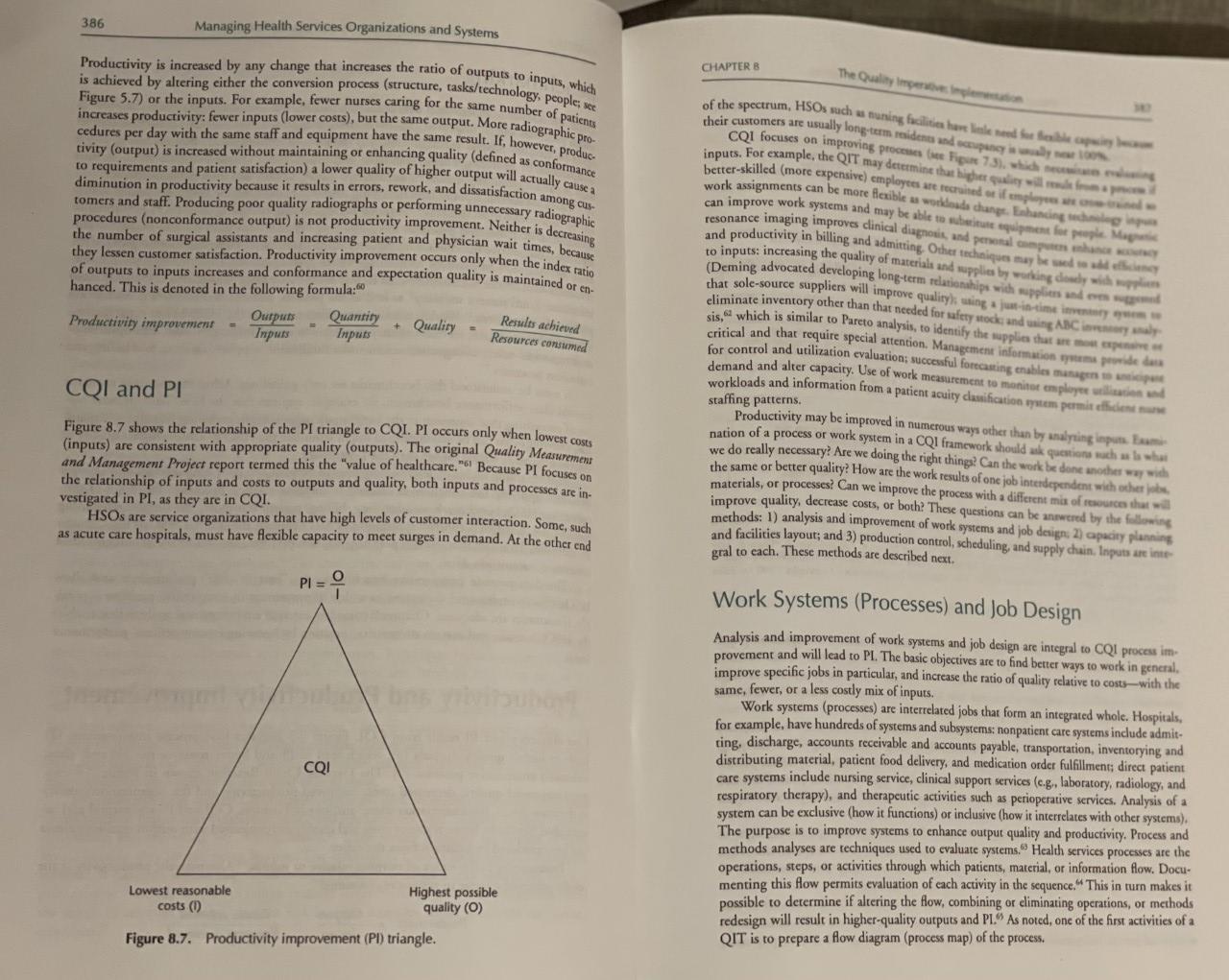
Help me, please
Please explain Answers in details
Controlling and Allocating Resources 575 CHAPTER 11 Case Study 3 Barriers to an Effective QI Effort District Hospital is a 260-bed, public, general acute care hospital owned by a special tax district . Its service area includes five communities with a total population of 180,000 in a southeastern coastal state in one of the nation's fastest-growing counties. It is one of three hos- pitals owned by the special tax district. The seven other hospitals in District Hospital's general service area make the environment highly competitive. District Hospital has a wide range of services and the active medical staff of 527 repre- sents most specialties. The emergency department (ED) is a major source of admissions. Last year, 26,153 patients visited the ED and 3,745, or 14.3%, were admitted. This was 42% of total hospital admissions. Some admissions were sent to the ED by private physicians and some came by ambulance, but most were self-referred. The hospital chief executive officer, W.G. Lester, noted that the number of visits to the ED was decreasing. Over a 3-year period, they had declined from a high of 29,345 to the current low of 26,153. Only part of this reduction seemed attributable to competition. Lester was also concerned about an increasing number of complaints concerning the quality of ED services. The complaints related to waiting time, poor attitudes of physicians, and questions about the quality of care. Investigation found that many complaints were justified, the causes of these problems were difficult to discern. Registered nurses (RN) employed in the ED want a larger role in triaging and treating patients, but the dominance of ED physicians limits the RNs' duties and frustrates other staff, as well. This is manifested among RN staff by high turnover, low morale, and difficulty in re- cruitment and retention. Another factor is the emergency medical technician (EMT) program started in the county a few years ago. The EMTs are an important community medical resource and are very influ- ential in deciding the hospital to which patients in ambulances will be transported. It will be necessary for District Hospital, through the ED physicians, to participate actively in training and managing the EMT program if District Hospital is to receive its share of emergency pa- tients. ED physicians have refused to participate in teaching or directing the program, however. In fact, they often alienate the EMTs. Lester is concerned, too, that the position of full-time director of emergency medicine at District Hospital has been vacant for 4 years. Residency programs in emergency medicine are producing physicians who are seeking positions with higher salaries and better working condi- tions than those available at District Hospital. There has been little turnover among the six physicians who staff the ED; they include one general surgeon (retired from private practice), two internists, and three non-U.S.-trained medical graduates with specialties in family practice. The ED physicians seem to lack a clear commitment to District Hospital . All of them contract separately with the hospital to provide ED services. District Hospital bills ED patients and collects the physicians' fees: moneys above the guaranteed minimum are paid to them pro rata. They participate in District Hospital's fringe benefits and are covered by its professional liability insurance policy. One ED physician, Dr. Balck (the retired surgeon), recognizes the progress being made nationally in emergency medicine. She made several unsuccessful attempts to move District Hospital in the same direction. With great effort, she instituted programs on intradepartmental education and mandatory attendance at approved courses in emergency medicine. Quality related activities, however , are done perfunctorily. Also, she has tried to obtain full recognition The members of the PSO seem satisfied with the situation. Its executive committee does not understand the changing status of emergency medicine. As evidence of its unwillingness to grant full recognition to the department, the PSO has consistently denied the ED's requests of the ED and its work by other members of the PSO. for full departmental status. 576 Managing Health Services Organizations and Systems Questions 1. Use the problem-solving methodology described in Chapter 6 to define the problem facing Lester. Which alternative solution should be implemented? Why? 2. Describe the relationship between inpatient census and ED admissions. Out- line a strategy to educate the members of the ED physician staff as to the relationship and importance of the ED to the financial good health of District Hospital. 3. Use the principles of CQI from Chapters 7 and 8 to outline a basic effort to improve quality in the ED. 4. Analyze the role of the EMTs and their relationship with District Hospital. What should be the role of ED physicians and staff at District Hospital in terms of educating the EMTs? What are the negative aspects of this educational activ- ity? Is there a potential conflict of interest? 5. Identify some control measures that could be used by Lester. 298 Managing Health Services Organizations and Systems Immediate CRISIS Prospective OPPORTUNITY THREAT WILL MIGHT Problem Solving Conditions HASSIS SEEK Retrospective DEVIATION Concurrent IMPROVEMENT Figure 6.3. Problem-solving conditions. onditionsbe sive marketing program may cause loss of market share. future results to be less than what is desired. For example, not responding to a competitor's aggres- Crisis problem solving is immediate. It responds to a current or predictable threat. Fail- ing to act promptly will cause untoward results, such as a decline in near-term performance. Examples of crisis problem solving are a local natural disaster, a wildcat strike by unionized employees, bypass equipment malfunction during surgery, or a sudden reduction in Medicaid Deviation problem solving is retrospective and occurs when actual and desired results payments. Loss of an essential employee may be a crisis. differ. Even small deviations may indicate large problems that must be clearly identified and solved. Improvement problem solving reduces the need for future deviation problem solving or improves performance . The perspective and process of continuous improvement differ from other problem-solving conditions in two important ways. First, continuous improvement is to support these efforts . This leads to continuously examining processes and seeking ways to improve them. Second, analysis is concurrent, broad based, and organizationwide and focuses on inputs and the conversion process. The management model in Figure 5.7 shows this Telas tionship . Improvement problem solving involves managers and staff as problem seekers who systematically seek opportunities for improvement. The condition of deviation is specifically referenced in the problem-solving process model that is depicted in Figure 6.4. The model is generic and is applicable to all problem solving except that conducted under the condition of improvement, where problem analysis differs. Historically , managers engaged most frequently in problem solving under conditions of de viation. The contemporary emphasis on quality and performance improvement, which is undertaken without a condition of deviation, is likely to make it the most common type of problem solving. Chapters 7 and 8 detail improvement problem solving. Managing 296 Ends- Means Nonprogrammable Administrative Programmable Operational Not Mutually Exclusive Figure 6.1. Types of decisions. more closely align with those desired. The process by which managers solve problems includes . the following: Selecting and analyzing a situation that requires a decision Developing and evaluating alternative solutions to address the situation Choosing an alternative (sometimes called decision analysis) Implementing the alternative Evaluating the results after implementation . Figure 6.2 shows the relationships among problem solving, problem analysis, and decision making. The terms problem solving and decision making are often used interchangeably but are not synonymous. All problem solving involves decision making (i.e., choosing among alterna- tives), but not all decision making involves problem solving." The distinction is that problem Predecision situation assessment Identifying and evaluating alternative solutions Decision Making Problem Solving Problem Analysis Alternative choice Postdecision alternative solution implementation and evaluation Figure 6.2. Problem solving and decision making. 336 Managing Health Services Organizations and Systems but also internal users of a department, a unit, or the outputs that an individual products CQI a customer is the person or process that relics on another person or proceso Output that is in conformance and meets the needs and expectations of customers is CQI, Productivity product or service and means that the HSO is doing the right things. Are We Doing Things Right? can be improved. "If it isn't perfect, make it better.*** Process improvement [2] is the second pillar of CQL. Output quality can be improved only by improving the processes that produce it. All processes can be improved. Improving processes in health services delivery is daunting because they are technical, complex, often intense, and are necessarily personal, intimate, and focused on individuals. These challenges have been and patient care systems from being improved. CQI means that even a process that functions well can be mer, however, and their high degree of dependence on human action does not preclude prove processes are continuous. Requisite to continuous improvement is developing a vys Finally, "doing things right requires that monitoring, evaluating, and intervening to im tematic understanding and documentation of processes. All staff must be trained in process improvement and encouraged to seek opportunities to improve work results by improving the way they are produced. The outcome is not only improved output quality (3) but also im proved productivity (4), in which there is more effective resource use, and enhanced competi- tive position [5]. Crosby urged organizations to establish a goal of "do it right the first time." This goal may be unattainable in an absolute sense, but HSOs that continuously improve Improvement, and Competitive Position The CQI paradigm is the recipe during the 1970s and into the 1980 the emphasis then was to the were narrowly applied. episodic, and then involvement and commitment and focus output quality. By contrast rather than simply long-term, and ongoing have extensive manager menti are customer driver and focus on improving the proces Figure 7.3 depicts the ways CQI improve quality competitive position (5). Deming asserted that does me improved quality results in PL The Deming Chain Reaction in Pa tionship: Better quality decreases costs, which improves productivity. In und decreased prices and increased market shares thus, the organization in jobs, and yields greater returns. Consequently, competitive position is en De argued that improved quality results in better resowe) processes mean less rework (readmissions), fewer mistakes (repeats of texts and feed (waiting for service). These results occur because the prospective and contro of, and changes made to work processes and inputs yield both improved quality and improved The Malcolm Baldrige National Quality Award (MBNQA), named for a US. of commerce who died while in office, was created in 1987 and has been awarded since 1988 The application process is rigorous, the award prestigious. Its purpose is to promote quality cellence; recognize organizations that have made significant improvements in product, service, productivity processes are moving in the "right" direction. How Can We Be Certain That We Do Things Right the First Time, Every Time? Decrease Improve quality of CQI (1) are as follows (see Figure 7.3): costs Improve productivity CQI has the goal of doing things right the first time, every time. If there is quality output the right things) and process improvement (doing things right) with CQI, the HSO/HS will move in the direction of doing things right the first time, every time (goal). The essential attributes CQI is an organizational philosophy that becomes pervasive in the culture the ingrained beliefs and values of the HSO/HS. It is customer driven and requires the transformation of CQI requires the total commitment and involvement of everyone in the HSO/HS. Man "gement must nurture the value system and commit the resources that support continuous improvement as integral to the work of everyone in the organization. Staff must partici pate in, and be committed to continuously improving their work results and the way those work units and departments. All staff must be involved in problem solving, especially to results are achieved. This requires collaboration and cross-functional coordination among existing beliefs and values regarding quality. Decrease prices Increase market Stay in business seek and identify opportunities for improvement. Enhance competitive position retrospective, it must be continuous, not intermittent. The aim is to prevent poor quality before it happens and to seek opportunities to improve processes in an organized fashion. Provide jobs and more jobs Return on investment age innovation, worker participation, and empowerment and build teams so that employ- Figure 7.4. Demine oli usati, 23. now we med one. Hos Town Cepation Management Hier New Business Consciousness, 23. New York McGraw-Hill, 1994; reprinted by permission of the McGraw-Hill Companies, Inc.) ons can contribute to proces improvement problem solving and facilitate organizations change that leads to improvement. 386 Managing Health Services Organizations and Systems CHAPTER B The Quality Productivity is increased by any change that increases the ratio of outputs to inputs, which is achieved by altering either the conversion process (structure, tasks/technology, people, see increases productivity: fewer inputs (lower costs), but the same output. More radiographic pro- Figure 5.7) or the inputs. For example, fewer nurses caring for the same number of patients cedures per day with the same staff and equipment have the same result. If, however, produc to requirements and patient satisfaction) a lower quality of higher output will actually cause a tivity (output) is increased without maintaining or enhancing quality (defined as conformance diminution in productivity because it results in errors, rework, and dissatisfaction among cus procedures (nonconformance output) is not productivity improvement. Neither is decreasing tomers and staff. Producing poor quality radiographs or performing unnecessary radiographic the number of surgical assistants and increasing patient and physician wait times, because CQI focuses more they lessen customer satisfaction. Productivity improvement occurs only when the index talice of outputs to inputs increases and conformance and expectation quality is maintained or en hanced. This is denoted in the following formula:60 Productivity improvement - Outputs Inputs Quantity Inputs + Quality - of the spectrum, HSOs such a tuning facilities have linie ned for being cam their customers are usually long-term residents and expany way to improving procemente Figure 73). inputs. For example, the QIT may determine that higher quality wil.com better-skilled (more expensive) employees are recruited if employees work assignments can be can improve work systems and may be able to whetinut equipment for people kupaca and productivity in billing and admitting Other techniques may be to inputs: increasing the quality of materials and supplies by working diamby widan Deming advocated developing long-term relationships with applies and even eliminate inventory other than that needed for safety rock and using ABC sis, which is similar to Pareto analysis, to identify the supplies that are expert critical and that require special attention. Management information tema de las for control and utilization evaluation: succesful forecasting enables managens demand and alter capacity. Use of work measurement to meninot employee will workloads and information from a patient acuity camification system permit eliciente Productivity may be improved in numerous ways other than by analyzing implum nation of a process or work system in a CQI framework should ask questions such as what we do really necessary? Are we doing the right things? Can the work be done another way with the same or better quality? How are the work results of one job interdependent with others materials, or processes? Can we improve the process with a different ma of resources that will improve quality, decrease costs, or both? These questions can be answered by the following methods: 1) analysis and improvement of work systems and job design. 2) apacity planning and facilities layout; and 3) production control, scheduling, and supply chain. Inputs are inte gral to cach. These methods are described next Results achieved Resources consumed CQI and PI staffing patterns. Figure 8.7 shows the relationship of the PI triangle to CQI. PI occurs only when lowest costs (inputs) are consistent with appropriate quality (outputs). The original Quality Measurement and Management Project report termed this the value of healthcare." Because PI focuses on the relationship of inputs and costs to outputs and quality, both inputs and processes are in- vestigated in PI, as they are in CQI. HSOs are service organizations that have high levels of customer interaction. Some, such as acute care hospitals, must have flexible capacity to meet surges in demand. At the other end PI = - Work Systems (Processes) and Job Design CQI Analysis and improvement of work systems and job design are integral to CQI process im- provement and will lead to Pl. The basic objectives are to find better ways to work in general improve specific jobs in particular, and increase the ratio of quality relative to costs-with the same, fewer, or a less costly mix of inputs. Work systems (processes) are interrelated jobs that form an integrated whole. Hospitals, for example, have hundreds of systems and subsystems: nonpatient care systems include admit- ting, discharge, accounts receivable and accounts payable, transportation, inventorying and distributing material, patient food delivery, and medication order fulfillment direct patient care systems include nursing service, clinical support services (c.g., laboratory, radiology, and respiratory therapy), and therapeutic activities such as perioperative services. Analysis of a system can be exclusive (how it functions) or inclusive (how it interrelates with other systems). The purpose is to improve systems to enhance output quality and productivity. Process and methods analyses are techniques used to evaluate systems. Health services processes are the operations, steps, or activities through which patients, material, or information flow. Docu- menting this Aow permits evaluation of each activity in the sequence. This in turn makes it possible to determine if altering the flow, combining or eliminating operations, or methods redesign will result in higher-quality outputs and PL. As noted, one of the first activities of a QIT is to prepare a flow diagram (process map) of the process. Lowest reasonable costs (1) Highest possible quality (0) Figure 8.7. Productivity improvement (Pl) triangleStep by Step Solution
There are 3 Steps involved in it
1 Expert Approved Answer
Step: 1 Unlock

Question Has Been Solved by an Expert!
Get step-by-step solutions from verified subject matter experts
Step: 2 Unlock
Step: 3 Unlock