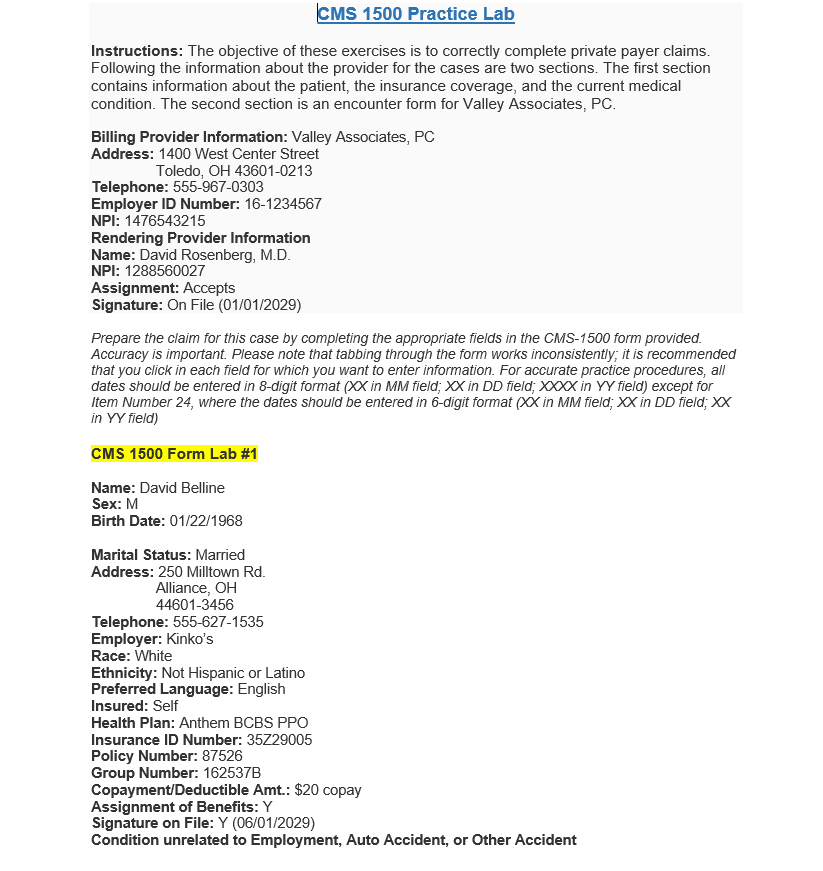
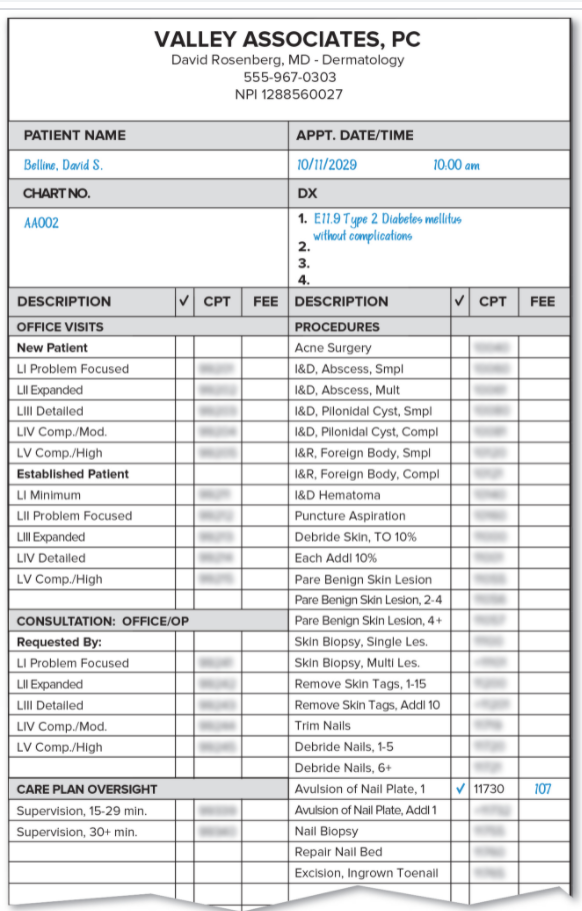
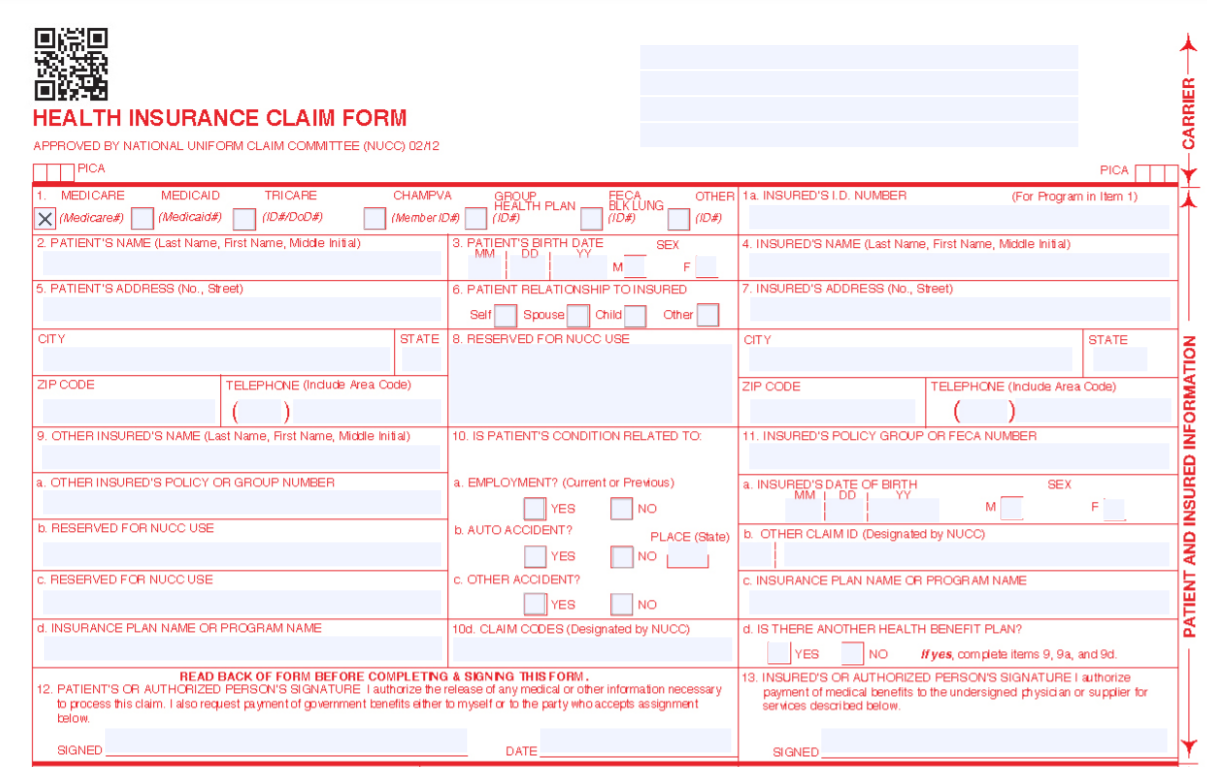
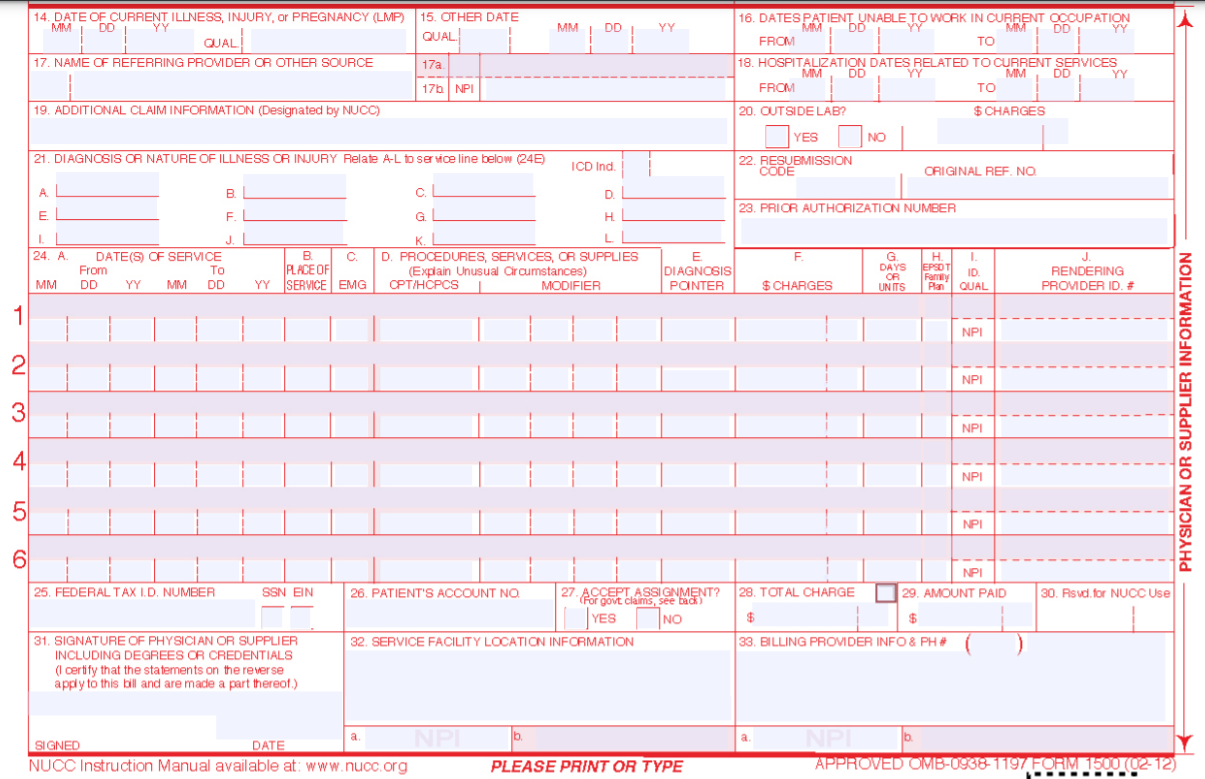
CMS 1500 Practice Lab Instructions: The objective of these exercises is to correctly complete private payer claims. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. Billing Provider Information: Valley Associates, PC Address: 1400 West Center Street Toledo, OH 43601-0213 Telephone: 555-967-0303 Employer ID Number: 16-1234567 NPI: 1476543215 Rendering Provider Information Name: David Rosenberg, M.D. NPI: 1288560027 Assignment: Accepts Signature: On File (01/01/2029) Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Please note that tabbing through the form works inconsistently, it is recommended that you click in each field for which you want to enter information. For accurate practice procedures, all dates should be entered in 8-digit format (XX in MM field; XX in DD field; XXXX in YY field) except for Item Number 24, where the dates should be entered in 6-digit format (XX in MM field; XX in DD field; XX in Yy field) CMS 1500 Form Lab #1 Name: David Belline Sex: M Birth Date: 01/22/1968 Marital Status: Married Address: 250 Milltown Rd. Alliance, OH 44601-3456 Telephone: 555-627-1535 Employer: Kinko's Race: White Ethnicity: Not Hispanic or Latino Preferred Language: English Insured: Self Health Plan: Anthem BCBS PPO Insurance ID Number: 35729005 Policy Number: 87526 Group Number: 162537B Copayment/Deductible Amt.: $20 copay Assignment of Benefits: Y Signature on File: Y (06/01/2029) Condition unrelated to Employment, Auto Accident, or Other Accident VALLEY ASSOCIATES, PC David Rosenberg, MD - Dermatology 555-967-0303 NPI 1288560027 PATIENT NAME Belline, David S. CHART NO. AA002 CPT FEE DESCRIPTION OFFICE VISITS New Patient LI Problem Focused LII Expanded LIII Detailed LIV Comp./Mod. LV Comp./High Established Patient LI Minimum LII Problem Focused LIII Expanded LIV Detailed LV Comp./High APPT. DATE/TIME 10/11/2029 10:00 am DX 1. E11.9 Type 2 Diabetes mellitus without complications 2. 3. 4. FEE DESCRIPTION CPT PROCEDURES Acne Surgery I&D, Abscess, Smp I&D, Abscess, Mult I&D, Pilonidal Cyst, Smpl I&D, Pilonidal Cyst, Compl I&R, Foreign Body, Smpl I&R, Foreign Body, Compl I&D Hematoma Puncture Aspiration Debride Skin, TO 10% Each Addi 10% Pare Benign Skin Lesion Pare Benign Skin Lesion, 2-4 Pare Benign Skin Lesion, 4+ Skin Biopsy, Single Les. Skin Blopsy, Multi Les Remove Skin Tags, 1-15 Remove Skin Tags, Addi 10 Trim Nails Debride Nails, 1-5 Debride Nails, 6+ Avulsion of Nail Plate, 1 11730 Avulsion of Nail Plate, Addl 1 Nail Biopsy Repair Nail Bed Excision, Ingrown Toenail CONSULTATION: OFFICE/OP Requested By: LI Problem Focused LII Expanded LIII Detailed LIV Comp./Mod. LV Comp./High 107 CARE PLAN OVERSIGHT Supervision, 15-29 min. Supervision, 30+ min. CARRIER HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE (NUCC) 0212 PICA 1 MEDICARE MEDICAID TRICARE CHAMPVA X Medicare#) Medicaid#) (ID#/D00#) (Member/D# PICATI OTHER 1a, INSURED'S I.D. NUMBER GROUP HEALTH PLAN (103) (For Program in Item 1) FECA BLK LUNG (ID# 2. PATIENT'S NAME (Last Name, First Name, Midde Inital) 4. INSURED'S NAME (Last Name, First Name, Middle Initia) 3. PATIENT'S BIRTH DATE SEX MMDD YY M F 6. PATIENT RELATIONSHIP TO INSURED 5. PATIENT'S ADDRESS (No., Street) 7. INSURED'S ADDRESS (No., Street) Other Self Spouse Child STATE 8. RESERVED FOR NUCC USE CITY CITY STATE ZIP CODE TELEPHONE (Indude Area Code) ZIP CODE TELEPHONE (Indude Area Code) ( ) 9. OTHER INSURED'S NAME (Last Name, First Name, Middle Initial) 10. IS PATIENT'S CONDITION RELATED TO 11. INSURED'S POLICY GROUP OR FECA NUMBER a. OTHER INSURED'S POLICY OR GROUP NUMBER a EMPLOYMENT? (Current or Previous) a. INSURED'S DATE OF BIRTH MM DD YY SEX PATIENT AND INSURED INFORMATION NO M F YES b. AUTO ACCIDENT? b. RESERVED FOR NUCC USE b. OTHER CLAIMID (Designated by NUCC) PLACE (State) NO C. RESERVED FOR NUCCUSE YES C. OTHER ACCIDENT? YES C. INSURANCE PLAN NAME OR PROGRAM NAME NO d. INSURANCE PLAN NAME OR PROGRAM NAME 10d. CLAIM CODES (Designated by NUCC) d. IS THERE ANOTHER HEALTH BENEFIT PLAN? YES NO yes, complete items 9, 9a, and 9d. 13. INSURED'S OR AUTHORIZED PERSON'S SIGNATURE I authorize payment of medical benefits to the undersigned physician or supplier for services described below. READ BACK OF FORM BEFORE COMPLETNG & SIGNNG THIS FORM 12. PATIENT'S OR AUTHORIZED PERSON'S SIGNATURE I authorize the release of any medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below SIGNED DATE SIGNED MM DD YY 14. DATE OF CURRENT ILLNESS, INJURY, or PREGNANCY (LMP) 15. OTHER DATE MM DD YY QUAL QUAL 17. NAME OF REFERRING PROVIDER OR OTHER SOURCE 17a. 17 NPI 19. ADDITIONAL CLAIM INFORMATION (Designated by NUCC) 16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION MM DD MM DD YY FROM TO 18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES MM DD YY MM DD YY FROM TO 20. OUTSIDE LAB? $ CHARGES $ YES NO 22. RESUBMISSION CODE ORIGINAL REF. NO 21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY Relate A-L to service line below (246) ICD Ind A B CL 23. PRIOR AUTHORIZATION NUMBER E F D G. . L D. PROCEDURES, SERVICES, OR SUPPLIES (Explain Unusual circumstances) CPT/HCPCS MODIFIER 24 A J DATE(S) OF SERVICE From To DD YY MM DD F . . PLACE OF YY SERVICE EMG E E DIAGNOSIS POINTER G DAYS OR UNITS H EPSOT Family Plan 1 ID QUAL J. RENDERING PROVIDER ID. + MM $ CHARGES 1 NPI NPI 2 3 PHYSICIAN OR SUPPLIER INFORMATION NPI 41 NPI 5 NPI 6 NPI 25. FEDERAL TAX ID. NUMBER SSN EIN 28. TOTAL CHARGE 29. AMOUNT PAID 30. Rsud. for NUCC Use 26. PATIENT'S ACCOUNT NO 27 ACCEPT ASSIGNMENT? (For govt claims, see back) NO 32. SERVICE FACILITY LOCATION INFORMATION YES $ 33. BILLING PROVIDER INFO & PH# 31. SIGNATURE OF PHYSICIAN OR SUPPLIER INCLUDING DEGREES OR CREDENTIALS (I certify that the statements on the reverse apply to this bill and are made a part thereof.) a b a b SIGNED DATE NP NUOC Instruction Manual available at: www.nucc.org PLEASE PRINT OR TYPE APPROVED OMB-0938 1197 FORM 150002-12)


