Question: || Directions with Performance Evaluation Checklist Study the EOB form in Workbook Figure 13-1, then calculate various figures and answer the following questions. 1st Attempt
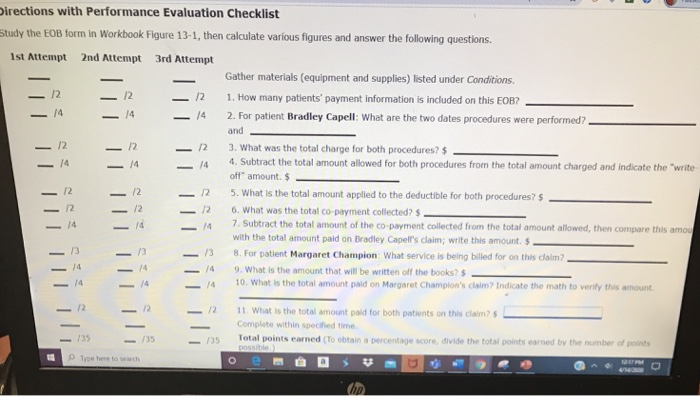
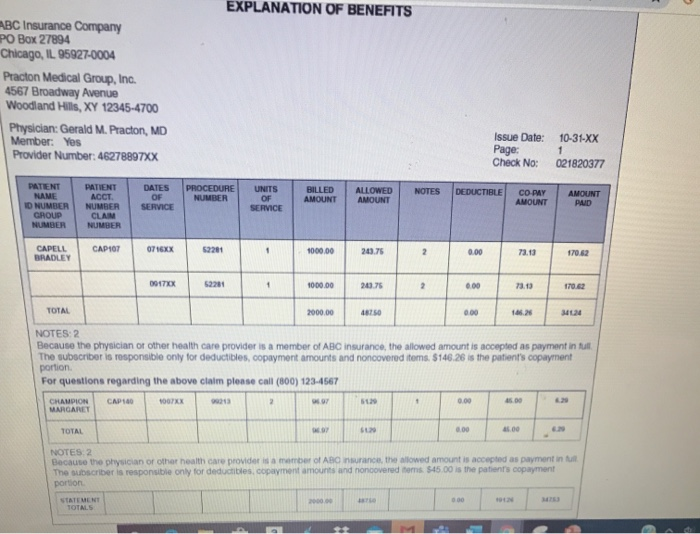
|| Directions with Performance Evaluation Checklist Study the EOB form in Workbook Figure 13-1, then calculate various figures and answer the following questions. 1st Attempt 2nd Attempt 3rd Attempt Gather materials (equipment and supplies) listed under Conditions. 1. How many patients' payment information is included on this EOB? 2. For patient Bradley Capell: What are the two dates procedures were performed? and 3. What was the total charge for both procedures? $ 4. Subtract the total amount allowed for both procedures from the total amount charged and indicate the "write off" amount. $ - 5. What is the total amount applied to the deductible for both procedures? $ 6. What was the total co-payment collected? $. 7. Subtract the total amount of the co-payment collected from the total amount allowed, then compare this amou with the total amount paid on Bradley Capell's claim; write this amount. $ 138 . For patient Margaret Champion: What service is being billed for on this claim? 9. What is the amount that will be written off the books? $ 4 10. What is the total amount paid on Margaret Champion's claim? Indicate the math to verify this amount 11! |||||||lli |||||ili TILLIT TIITTI 12 11 What is the total amount paid for both patients on this claims Complete within specified time Total points earned (To obtain a percentage score, divide the total points earned by the number of points possible) 35 Tyhetsch EXPLANATION OF BENEFITS BC Insurance Company PO Box 27894 Chicago, IL 95927-0004 Practon Medical Group, Inc. 4567 Broadway Avenue Woodland Hills, XY 12345-4700 Physician: Gerald M. Practon, MD Member: Yes Provider Number: 46278897XX Issue Date: Page: Check No: 10-31-XX 021820377 PROCEDURE NUMBER AMOUNT NOTES BILLED AMOUNT DEDUCTIBLE DATES OF SERVICE ALLOWED AMOUNT UNITS OF SERVICE PATIENT NANE ID NUMBER CROUD NUMBER COPY AMOUNT PATIENT ACCT NUMBER CLAN NUMBER PAD CAPELL BRADLEY OT 16XX 52201 1000.00 20.75 73.13 170.62 TOX 1000.00 2007 10.02 TOTAL 00000 NOTES: 2 Because the physician of other health care provider is a member of ABC insurance, the allowed amount is accepted as payment in full The subscriber is responsible only for deductibles, copayment amounts and noncovered toms. $146.26 is the patient's copayment portion For questions regarding the above claim please call (800) 123-4567 CHAMPION CAP 1007 MARGARET TOTAL NOTES 2 Because the physican or other health care providers a mber of A n urance the wed amount is accepted as payment The subscriber is responsible only for deducities, oopment amounts and noncovered ms 545.00 Is the patient's copayment portion STATEMENT || Directions with Performance Evaluation Checklist Study the EOB form in Workbook Figure 13-1, then calculate various figures and answer the following questions. 1st Attempt 2nd Attempt 3rd Attempt Gather materials (equipment and supplies) listed under Conditions. 1. How many patients' payment information is included on this EOB? 2. For patient Bradley Capell: What are the two dates procedures were performed? and 3. What was the total charge for both procedures? $ 4. Subtract the total amount allowed for both procedures from the total amount charged and indicate the "write off" amount. $ - 5. What is the total amount applied to the deductible for both procedures? $ 6. What was the total co-payment collected? $. 7. Subtract the total amount of the co-payment collected from the total amount allowed, then compare this amou with the total amount paid on Bradley Capell's claim; write this amount. $ 138 . For patient Margaret Champion: What service is being billed for on this claim? 9. What is the amount that will be written off the books? $ 4 10. What is the total amount paid on Margaret Champion's claim? Indicate the math to verify this amount 11! |||||||lli |||||ili TILLIT TIITTI 12 11 What is the total amount paid for both patients on this claims Complete within specified time Total points earned (To obtain a percentage score, divide the total points earned by the number of points possible) 35 Tyhetsch EXPLANATION OF BENEFITS BC Insurance Company PO Box 27894 Chicago, IL 95927-0004 Practon Medical Group, Inc. 4567 Broadway Avenue Woodland Hills, XY 12345-4700 Physician: Gerald M. Practon, MD Member: Yes Provider Number: 46278897XX Issue Date: Page: Check No: 10-31-XX 021820377 PROCEDURE NUMBER AMOUNT NOTES BILLED AMOUNT DEDUCTIBLE DATES OF SERVICE ALLOWED AMOUNT UNITS OF SERVICE PATIENT NANE ID NUMBER CROUD NUMBER COPY AMOUNT PATIENT ACCT NUMBER CLAN NUMBER PAD CAPELL BRADLEY OT 16XX 52201 1000.00 20.75 73.13 170.62 TOX 1000.00 2007 10.02 TOTAL 00000 NOTES: 2 Because the physician of other health care provider is a member of ABC insurance, the allowed amount is accepted as payment in full The subscriber is responsible only for deductibles, copayment amounts and noncovered toms. $146.26 is the patient's copayment portion For questions regarding the above claim please call (800) 123-4567 CHAMPION CAP 1007 MARGARET TOTAL NOTES 2 Because the physican or other health care providers a mber of A n urance the wed amount is accepted as payment The subscriber is responsible only for deducities, oopment amounts and noncovered ms 545.00 Is the patient's copayment portion STATEMENT