

Question: Reference the case. sales force management at Nobel llac . Answer following Identify the facets related to recruitment and training that were root cause to
Reference the case. sales force management at Nobel llac . Answer following
- Identify the facets related to recruitment and training that were root cause to high employee turnover
- Critically apraise compensation plan of company
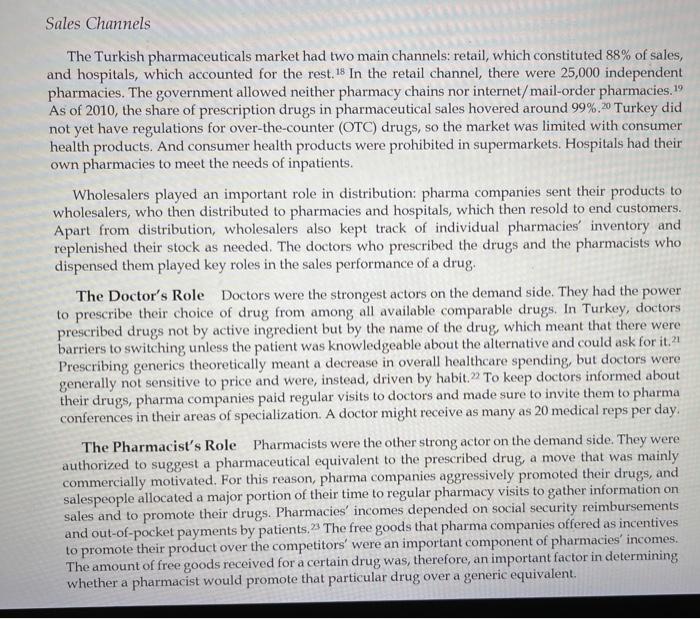
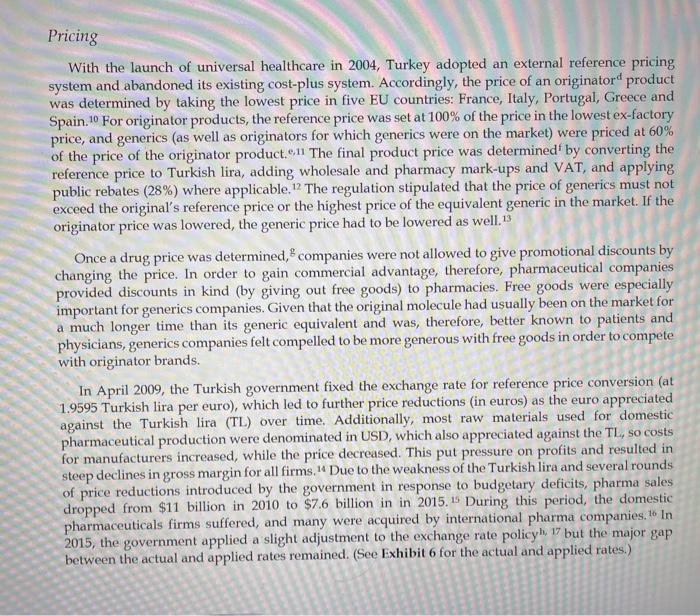
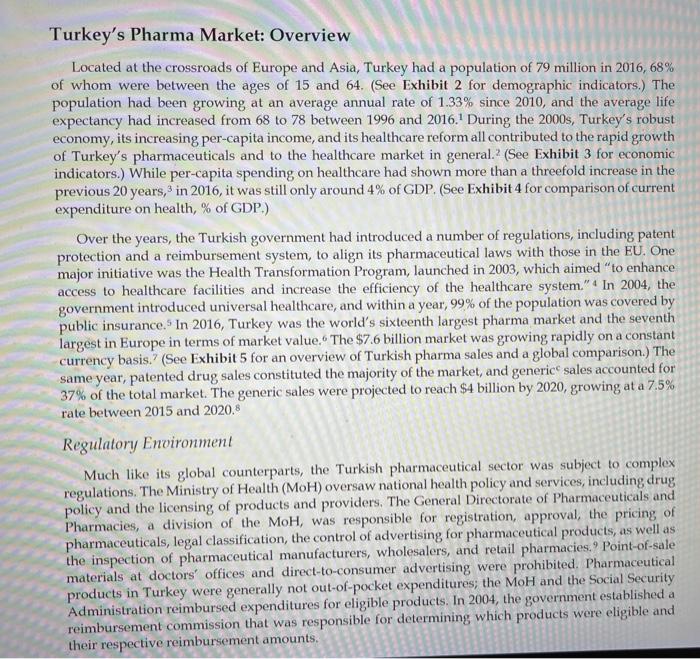
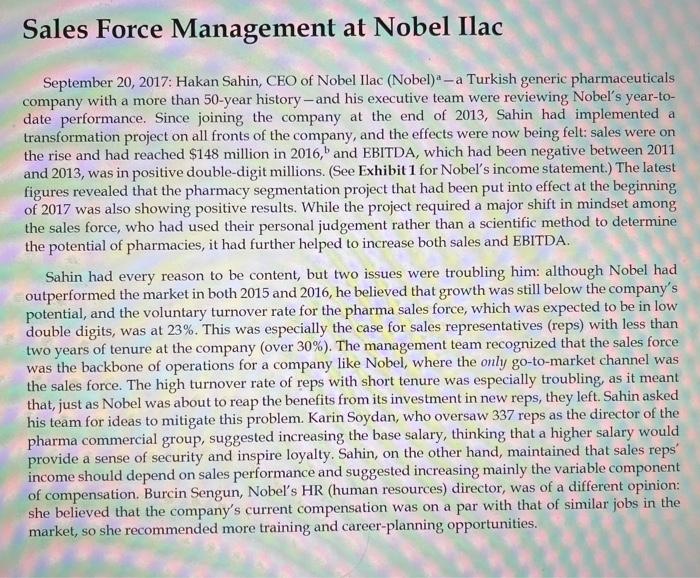
The Turkish pharmaceuticals market had two main channels: retail, which constituted 88% of sales, and hospitals, which accounted for the rest. 18 In the retail channel, there were 25,000 independent pharmacies. The government allowed neither pharmacy chains nor internet/mail-order pharmacies. 19 As of 2010, the share of prescription drugs in pharmaceutical sales hovered around 99%.20 Turkey did not yet have regulations for over-the-counter (OTC) drugs, so the market was limited with consumer health products. And consumer health products were prohibited in supermarkets. Hospitals had their own pharmacies to meet the needs of inpatients. Wholesalers played an important role in distribution: pharma companies sent their products to wholesalers, who then distributed to pharmacies and hospitals, which then resold to end customers. Apart from distribution, wholesalers also kept track of individual pharmacies' inventory and replenished their stock as needed. The doctors who prescribed the drugs and the pharmacists who dispensed them played key roles in the sales performance of a drug. The Doctor's Role Doctors were the strongest actors on the demand side. They had the power to prescribe their choice of drug from among all available comparable drugs. In Turkey, doctors prescribed drugs not by active ingredient but by the name of the drug, which meant that there were barriers to switching unless the patient was knowledgeable about the alternative and could ask for it. 21 Prescribing generics theoretically meant a decrease in overall healthcare spending, but doctors were generally not sensitive to price and were, instead, driven by habit. 2 To keep doctors informed about their drugs, pharma companies paid regular visits to doctors and made sure to invite them to pharma conferences in their areas of specialization. A doctor might receive as many as 20 medical reps per day. The Pharmacist's Role Pharmacists were the other strong actor on the demand side. They were authorized to suggest a pharmaceutical equivalent to the prescribed drug, a move that was mainly commercially motivated. For this reason, pharma companies aggressively promoted their drugs, and salespeople allocated a major portion of their time to regular pharmacy visits to gather information on sales and to promote their drugs. Pharmacies' incomes depended on social security reimbursements and out-of-pocket payments by patients, 23 The free goods that pharma companies offered as incentives to promote their product over the competitors' were an important component of pharmacies' incomes. The amount of free goods received for a certain drug was, therefore, an important factor in determining whether a pharmacist would promote that particular drug over a generic equivalent. With the launch of universal healthcare in 2004, Turkey adopted an external reference pricing system and abandoned its existing cost-plus system. Accordingly, the price of an originator d product was determined by taking the lowest price in five EU countries: France, Italy, Portugal, Greece and Spain. 10 For originator products, the reference price was set at 100% of the price in the lowest ex-factory price, and generics (as well as originators for which generics were on the market) were priced at 60% of the price of the originator product. .11 The final product price was determined by converting the reference price to Turkish lira, adding wholesale and pharmacy mark-ups and VAT, and applying public rebates (28% ) where applicable. 12 The regulation stipulated that the price of generics must not exceed the original's reference price or the highest price of the equivalent generic in the market. If the originator price was lowered, the generic price had to be lowered as well. 13 Once a drug price was determined, g companies were not allowed to give promotional discounts by changing the price. In order to gain commercial advantage, therefore, pharmaceutical companies provided discounts in kind (by giving out free goods) to pharmacies. Free goods were especially important for generics companies. Given that the original molecule had usually been on the market for a much longer time than its generic equivalent and was, therefore, better known to patients and physicians, generics companies felt compelled to be more generous with free goods in order to compete with originator brands. In April 2009, the Turkish government fixed the exchange rate for reference price conversion (at 1.9595 Turkish lira per euro), which led to further price reductions (in euros) as the euro appreciated against the Turkish lira (TL) over time. Additionally, most raw materials used for domestic pharmaceutical production were denominated in USD, which also appreciated against the TL, so costs for manufacturers increased, while the price decreased. This put pressure on profits and resulted in steep declines in gross margin for all firms. 14 Due to the weakness of the Turkish lira and several rounds of price reductions introduced by the government in response to budgetary deficits, pharma sales dropped from $11 billion in 2010 to $7.6 billion in in 2015.15 During this period, the domestic pharmaceuticals firms suffered, and many were acquired by international pharma companies. 16 In 2015, the government applied a slight adjustment to the exchange rate policy h17 but the major gap between the actual and applied rates remained. (See Exhibit 6 for the actual and applied rates.) Located at the crossroads of Europe and Asia, Turkey had a population of 79 million in 2016, 68% of whom were between the ages of 15 and 64. (See Exhibit 2 for demographic indicators.) The population had been growing at an average annual rate of 1.33% since 2010, and the average life expectancy had increased from 68 to 78 between 1996 and 2016.1 During the 2000s, Turkey's robust economy, its increasing per-capita income, and its healthcare reform all contributed to the rapid growth of Turkey's pharmaceuticals and to the healthcare market in general.2 (See Exhibit 3 for economic indicators.) While per-capita spending on healthcare had shown more than a threefold increase in the previous 20 years, 3 in 2016 , it was still only around 4% of GDP. (See Exhibit 4 for comparison of current expenditure on health, % of GDP.) Over the years, the Turkish government had introduced a number of regulations, including patent protection and a reimbursement system, to align its pharmaceutical laws with those in the EU. One major initiative was the Health Transformation Program, launched in 2003, which aimed "to enhance access to healthcare facilities and increase the efficiency of the healthcare system." 4 In 2004, the government introduced universal healthcare, and within a year, 99% of the population was covered by public insurance. 5 In 2016, Turkey was the world's sixteenth largest pharma market and the seventh largest in Europe in terms of market value 6 The $7.6 billion market was growing rapidly on a constant currency basis.? (See Exhibit 5 for an overview of Turkish pharma sales and a global comparison.) The same year, patented drug sales constituted the majority of the market, and genericc sales accounted for 37% of the total market. The generic sales were projected to reach $4 billion by 2020 , growing at a 7.5% rate between 2015 and 2020.8 Regulatory Environment Much like its global counterparts, the Turkish pharmaceutical sector was subject to complex regulations. The Ministry of Health (MoH) oversaw national health policy and services, including drug policy and the licensing of products and providers. The General Directorate of Pharmaceuticals and Pharmacies, a division of the MoH, was responsible for registration, approval, the pricing of pharmaceuticals, legal classification, the control of advertising for pharmaceutical products, as well as the inspection of pharmaceutical manufacturers, wholesalers, and retail pharmacies.? Point-of-sale materials at doctors' offices and direct-to-consumer advertising were prohibited. Pharmaceutical products in Turkey were generally not out-of-pocket expenditures; the MoH and the Social Security Administration reimbursed expenditures for eligible products. In 2004, the government established a reimbursement commission that was responsible for determining which products were eligible and September 20, 2017: Hakan Sahin, CEO of Nobel Ilac (Nobel) - a Turkish generic pharmaceuticals company with a more than 50-year history - and his executive team were reviewing Nobel's year-todate performance. Since joining the company at the end of 2013, Sahin had implemented a transformation project on all fronts of the company, and the effects were now being felt: sales were on the rise and had reached $148 million in 2016,, and EBITDA, which had been negative between 2011 and 2013, was in positive double-digit millions. (See Exhibit 1 for Nobel's income statement.) The latest figures revealed that the pharmacy segmentation project that had been put into effect at the beginning of 2017 was also showing positive results. While the project required a major shift in mindset among the sales force, who had used their personal judgement rather than a scientific method to determine the potential of pharmacies, it had further helped to increase both sales and EBITDA. Sahin had every reason to be content, but two issues were troubling him: although Nobel had outperformed the market in both 2015 and 2016, he believed that growth was still below the company's potential, and the voluntary turnover rate for the pharma sales force, which was expected to be in low double digits, was at 23%. This was especially the case for sales representatives (reps) with less than two years of tenure at the company (over 30% ). The management team recognized that the sales force was the backbone of operations for a company like Nobel, where the only go-to-market channel was the sales force. The high turnover rate of reps with short tenure was especially troubling, as it meant that, just as Nobel was about to reap the benefits from its investment in new reps, they left. Sahin asked his team for ideas to mitigate this problem. Karin Soydan, who oversaw 337 reps as the director of the pharma commercial group, suggested increasing the base salary, thinking that a higher salary would provide a sense of security and inspire loyalty. Sahin, on the other hand, maintained that sales reps' income should depend on sales performance and suggested increasing mainly the variable component of compensation. Burcin Sengun, Nobel's HR (human resources) director, was of a different opinion: she believed that the company's current compensation was on a par with that of similar jobs in the market, so she recommended more training and career-planning opportunities
Step by Step Solution
There are 3 Steps involved in it

Get step-by-step solutions from verified subject matter experts