

Question: Community Hospital Part I: Answer each question thoroughly, read over each problem, discuss the pros and cons of each option, and select the best option
Community Hospital
Part I: Answer each question thoroughly, read over each problem, discuss the pros and cons of each option, and select the best option including your justification.
Community Hospital is a 200-bed care hospital located in a Midwestern city with a population of 300,000. The hospital was founded 25 years ago by a group of local residents. The hospital started as an 80-bed facility and has since grown to a 200-bed modern health care center. The founding physicians sold their interest in Community Hospital to United Healthcare, Inc., 10 years later. Community Hospital was one of Uniteds early acquisitions, and in the 15 years since its purchase, both Community and United Healthcare have exhibited healthy growth.
Although Community Hospital has grown over the years, it has always had a reputation for providing warm and attentive care to patients. The staff has been proud of its reputation and seeks to give individual attention to patients. Approximately 400 people are employed to meet the staffing needs of the hospital. The largest percentage of hospital staff are employed in one of the many nursing service departments. The food and nutrition department and housekeeping department employ an equal number of employees to support the patient care services of other departments.
The individual departments are managed by a department head who reports to either the assistant administrator, director of nursing, or controller. Each department functions as a separate unit and department heads make many autonomous decisions regarding their operations. For successful operations, individual departments must work together and depend on each other in order to provide good patient care. An example of this interdependence is seen everyday in providing meals for the patients. The food and nutrition department prepares the food and patient trays, and the nursing unit is responsible for passing the trays to patients and returning them to the cart for delivery back to the food and nutrition department. The top priority of each hospital department should be to provide good patient care whether directly or indirectly. Communications between departments must be maintained in order to facilitate patient care. An organizational chart of the hospital is presented in Figure 1.
Competition
Community Hospital is located in a very aggressive health care market. Its major competition is a City Hospital, which is a 500-bed medical center located in the downtown area. City Hospital is affiliated with the local medical school and offers some services unavailable at Community Hospital. City Hospital is also a public hospital versus Communitys for-profit status.
City Hospital has a strong marketing emphasis, which includes advertising in print and television. It offers seminars for the public on current medical issues of interest to develop their patient base. To increase public awareness, Community Hospital has begun marketing efforts with billboards and print advertising.
Community Hospital must not only compete for patients but also physicians. Almost all of the citys 250 physicians have privileges to admit patients at City Hospital. Community Hospital has approximately 75 physicians who actively admit patients and use the hospitals services. Of the remaining 175 physicians, 100 use Community Hospital occasionally, and the remaining 75 do not admit patients at all. Some of the reasons that physicians do not use Community Hospital are because it is located away from the traditional medical district and lacks some types of medical equipment and services.
To counteract these deficiencies, a new administrator was brought into Community Hospital from United Healthcare. His primary goal was to develop stronger bonds between the physician and hospital. Several new pieces of medical equipment have been purchased to upgrade services. Construction has been completed on several medical office buildings in order to bring the physicians closer to Community Hospital. It should be noted that physicians often make the choice when deciding on the hospital for admission, especially when they limit their practice to one facility. Therefore, it is important for hospitals to develop strong and loyal ties with physicians to attract their business.
Trends in the Health Care Industry
The increasing cost of health care is causing tremendous changes for health care providers. New technology in medical equipment causes equipment to become obsolete and necessitates replacements with large capital outlays. The rising cost of health care has had a tremendous impact on insurance companies. With escalating costs, individuals are asked to pay a larger deductible and many employers are decreasing the benefits for which they are insuring employees.
Out-patient procedures are increasing to help decrease medical costs. This has hurt hospitals because occupancy rates are declining. In 1984, Medicare instituted a monumental change in the way that they reimburse hospitals for care given to their participants (those over 65). The new system, diagnostic-related groups (DRG) pays a fixed payment based on the average cost of caring for a patient with a particular diagnosis. Before DRG, hospitals were reimbursed for the charges made during the patients length of stay in the hospital. With the inception of the DRG, shorter hospital stays have decreased patient occupancy rates. When patients must stay past the length of stay approved by Medicare, the hospital must absorb the costs not covered. Many private insurance firms are requiring that participants be approved for admission to the hospital in order to decrease unnecessary hospital stays in an effort to reduce costs.
Gone are the days when hospitals did not have to be concerned with their cost of operations. With declining patient census, hospitals are expanding into out-patient services to increase utilization of hospital services. Many hospitals have undergone reductions in staffing to decrease labor costs as occupancy rates have declined. Hospitals are coping with revenue changes and expanding into new areas to seek opportunities.
Community Hospital has been affected only slightly by the declining occupancy rates. This can be attributed to the newly opened physicians office building nearby and the healthy economy of the area. Other hospitals in United Healthcare have not been so fortunate, and many have had significant staffing reductions to counteract their decreased usage.
Food and Nutrition Services
The food and nutrition services department will be the focus of the study of the study of Community Hospital. There are currently 30 FTEs (full-time equivalents employed in the department. The department has lost two FTEs by phasing out positions when employees resigned and by shifting some job responsibilities. Employees have also been cross-trained so that they are able to perform several jobs. This makes the employees more useful and this versatility eases scheduling. These efforts have been made in order to help control the labor costs of the department. Labor costs account for over 50 percent of the food and nutrition services departments costs and average $320,000 per year. Food costs run a close second with approximately $300,000 spent per year on food. The food and nutrition services department is considered a cost center in the hospital, although efforts are being made to increase revenue through the cafeteria and with nutrition services such as out-patient diet counseling.
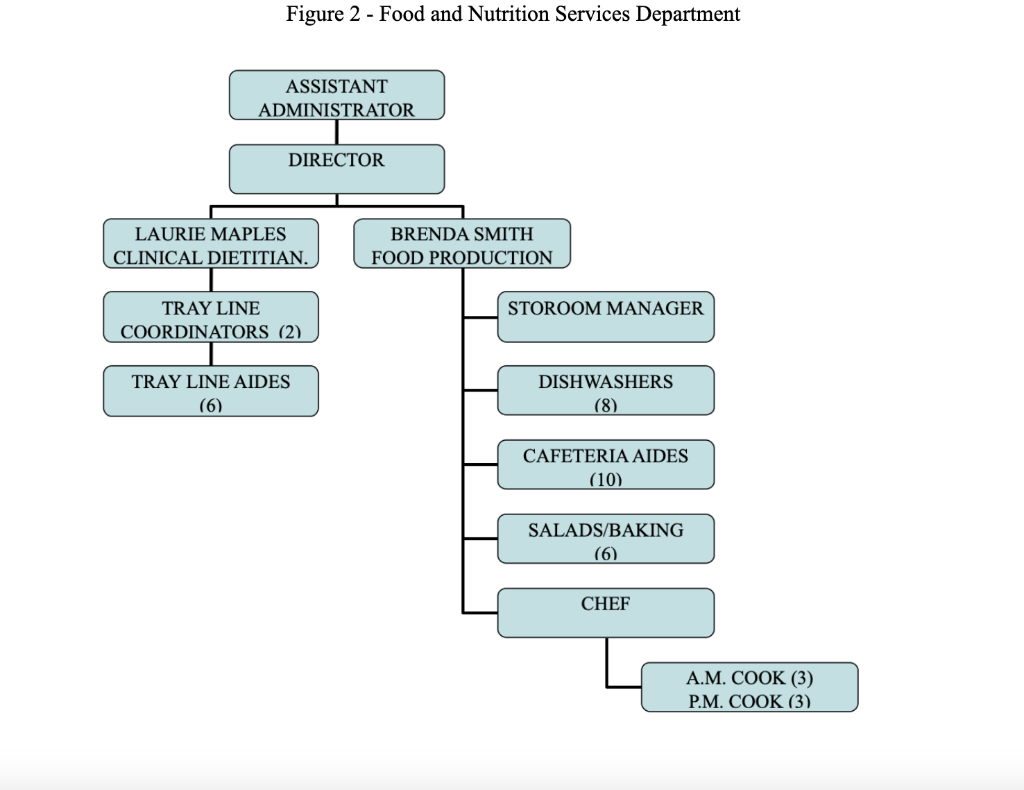
The director of the food and nutrition services department is assisted by Laurie Maples, the clinical dietitian, and Brenda Smith, the food production supervisor. Laurie Maples has recently graduated from college and is a newly registered dietitian or R.D. Brenda Smith is a long-time employee of Community Hospital. She has worked her way up from tray line aide to her current position as food production supervisor. Figure 2 presents the organization chart of the food and nutrition services department.
The department is responsible for meal preparation and service to patients and cafeteria patrons. Approximately 700 meals are served each day. The department is in operation from 5:30 a.m. to 7:30 p.m. daily. Three meals per day are served in the cafeteria and to patients. In addition, some catering is performed, ranging from breakfasts and luncheons to cookies and coffee for a meeting.
The department is split into two areas of responsibility: nutritional care of patients and food production. The clinical dietitian is responsible for the nutritional care of patients, which includes assessment of patients nutritional needs, education of patients on modified diets, and monitoring food intake and tolerance. The clinical dietitian spends 80 percent of her time away from the department seeing patients on the various nursing units. The tray line coordinators oversee the preparation of patient trays, set up patient menus for meal service, answer phones, and note diet changes for the clinical dietitian. The tray line aides job responsibilities include setting up the patient tray line for service of patient trays and stocking each station on the tray line. They assist the dishwashers when the patient trays are returned to the kitchen and put away clean dishes and silverware. The patient tray line can be thought of as a mini-assembly line, with six stations where particular food items are placed on the patient tray. It takes about 30 to 45 minutes to prepare the patient trays for one meal. The tray line is in operation three times per day every day of the week. When the patient food service is completed, food is put away to use for late patient trays, and the stations are restocked.
As food production supervisor, Brenda Smith is responsible for food purchasing and production, sanitation, and cafeteria operations. The storeroom manager is responsible for food purchasing and storage, with Brenda overseeing this area. Menus are the critical part of the operation because they define production needs. The director is responsible for writing the menus for the patients and cafeteria. The chef oversees the cooking efforts of the a.m. cook, who prepares breakfast for the cafeteria and patients and also assists the chef with lunch preparation. The p.m. cook prepares the supper meal for patients and the cafeteria, with assistance from the chef. The baker is responsible for preparing baked goods for cafeteria and patient meals. The salad maker has similar responsibilities with salad preparation in addition to the salad bar in the cafeteria. Three dishwashers are normally assigned each day. The first dishwasher comes in at 6:30 a.m. and is responsible for washing dishes. The second dishwasher comes in at 9:00 a.m. and is responsible for washing pots and pans. The third dishwasher comes to work at 1:00 and is responsible for dishwashing and special cleaning assignments in the afternoon.
The last area under Brenda Smiths supervision is the cafeteria. Two employees work in the cafeteriaan early aide is assigned to work breakfast and lunch, and a late cafeteria aide is assigned to work lunch and supper. Lunch meal service is the busiest meal in the cafeteria and requires two employees to serve the customers. Cafeteria aides are responsible for cleaning and restocking the cafeteria with food items and dishes between meals.
Lines of responsibility cross between patient nutrition care and food production. There are many areas of both the patients and cafeteria, but Laurie Maples is responsible for patient food service and Brenda Smith for cafeteria food service. This structure sometimes leads to confusion.
The top priority of the food and nutrition services department is preparing quality food. The needs of the patients rank above those of the cafeteria. The department has a reputation for preparing good food for the patients and cafeteria. Laurie Maples is responsible for ensuring that patients receive the correct food items served at the proper food temperature. This is especially important for patients who require modifications of their diet due to illness or disease. Forty percent of the patients in the hospital receive a modified diet. Many other patients need adjustments to the regular diet so that it is similar to what they are accustomed to eating.
Recently there have been a number of problems in the department. Janice Livingston has resigned as director. You have been hired as the new director and part of your responsibilities will be to address some of these problems.
Figure 1: Community Hospital
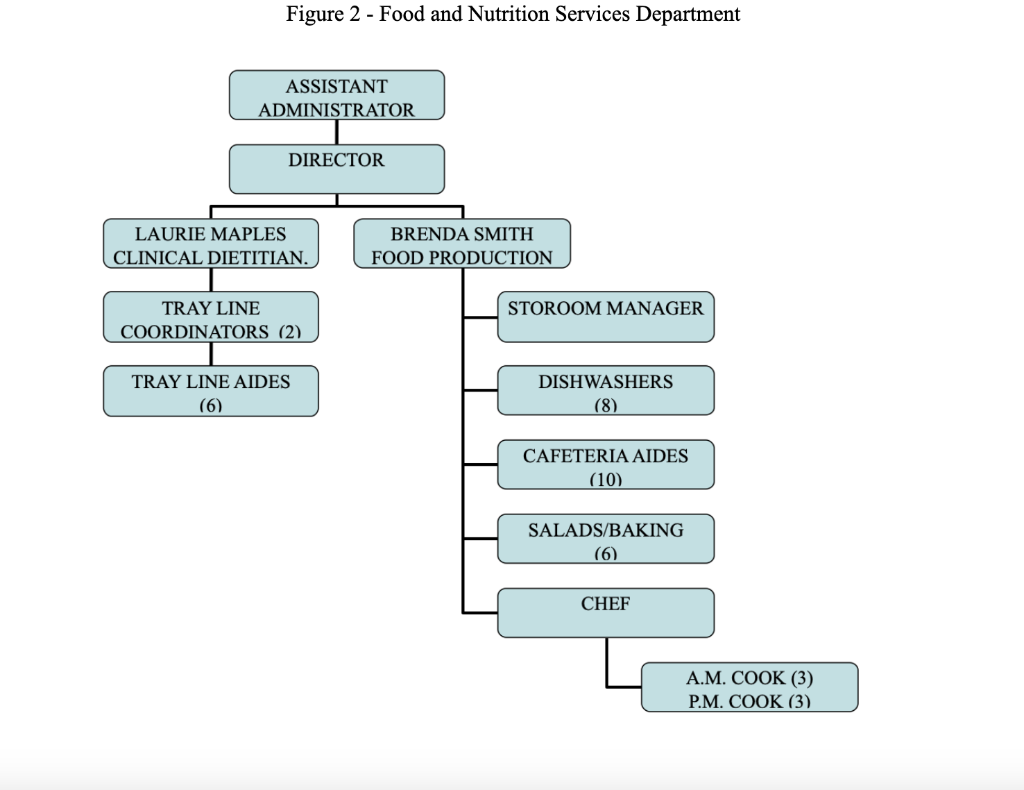
Figure 2 - Food and Nutrition Services Department
Part II: Analysis Questions Answer the following completely:
1. Why should Community Hospital be concerned with DRG? Discuss
2. What is the span of control for each individual in Figure 1?
3. What type of departmentalization is being used? Discuss.
4. How can the organizational chart depicted in Figure 1 be organized more effectively? Draw a new organizational chart and discuss each change.
5. What is the span of control for each supervisor in Figure 2?
6. How can the organizational chart depicted in Figure 2 be organized more effectively? Draw a new organizational chart and discuss each change.
7. What behavior modification technique could be used on John to control his behavior? Discuss.
8. What type of competition is Community Hospital engaged in? Discuss.
9. What elements comprise the companys promotion mix.
Figure 2 - Food and Nutrition Services Department Figure 2 - Food and Nutrition Services Department
Step by Step Solution
There are 3 Steps involved in it

Get step-by-step solutions from verified subject matter experts